
Anal fissure symptoms are often distinctive and severe. Recognizing them early helps guide correct treatment. For full management options, see anal fissure treatment in Dubai.
Understanding this mechanism helps explain why dietary changes alone are often not enough, why topical creams work the way they do, and why surgery achieves such high cure rates.
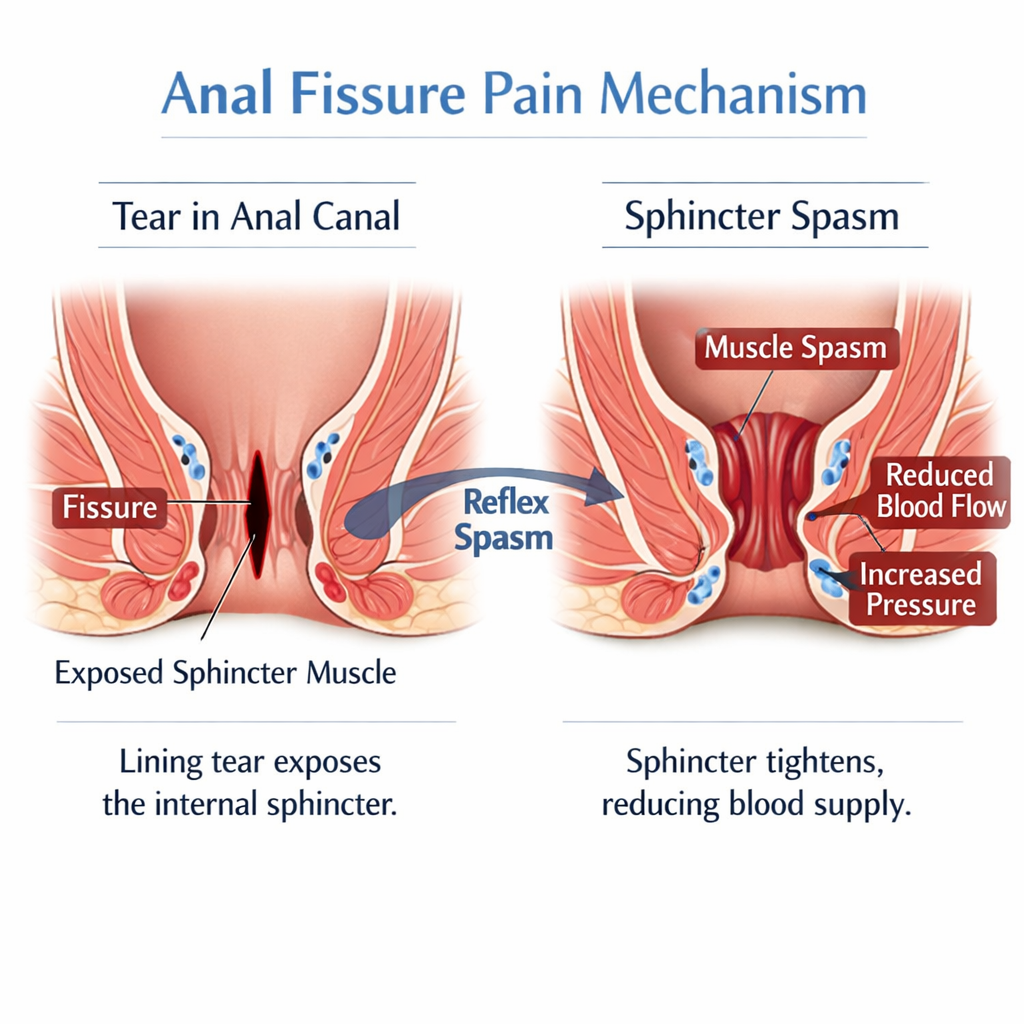
Step 1: The Tear
The anal canal lining tears — usually at the posterior midline — when stretched by a hard or large stool. This exposes the underlying internal anal sphincter.
Step 2: Reflex Sphincter Spasm
The internal anal sphincter is an involuntary muscle – you cannot consciously control it. When the lining tears and the sphincter is exposed or stimulated, it responds by contracting – going into spasm.
This is a protective reflex. The problem is that it is counterproductive in the context of a fissure:
- The spasm increases pressure inside the anal canal
- This increased pressure further compresses the blood vessels supplying the posterior midline
- The posterior midline already has relatively poor blood supply compared to other parts of the anal canal
- Reduced blood supply means the tear cannot heal
- Failure to heal means the spasm continues — a self-perpetuating cycle
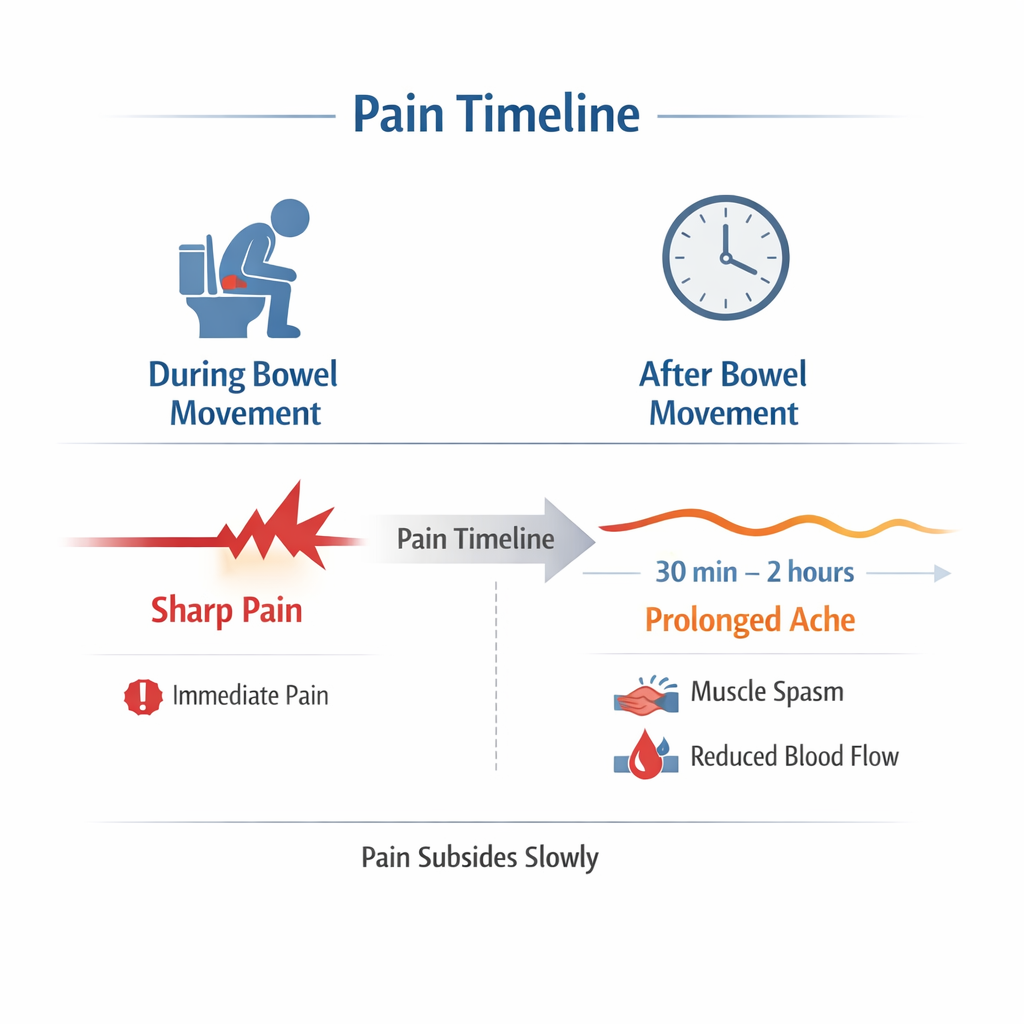
Step 3: Ischemic Pain
The prolonged pain after a bowel movement — the pain that continues for 30 minutes, an hour, sometimes two hours — is not just from the tear. It is largely ischemic: the spastic sphincter is cutting off blood supply to the posterior midline, causing pain similar to a muscle cramp or angina.
Why This Matters for Treatment
Dietary Changes
Softer stools reduce the tear-triggering stimulus. This helps prevent new tears and reduces the severity of each episode — but it does not break the spasm-ischemia cycle if a chronic fissure is already established.
Topical Creams (GTN, Diltiazem)
These work by relaxing the internal sphincter – reducing spasm, improving blood supply, and creating conditions in which healing can occur. They target the mechanism, not just the symptoms.
Botox Injection
Botox injection for anal fissure in Dubai temporarily paralyses part of the internal sphincter, eliminating spasm for 2–4 months – long enough for most fissures to heal.
Lateral Internal Sphincterotomy
Lateral internal sphincterotomy in Dubai permanently eliminates the pathological spasm by dividing part of the internal sphincter. This is why LIS has a >95% healing rate – it directly addresses the underlying cause.
When Is Severe Anal Pain Not a Fissure?
- Thrombosed external hemorrhoid: Constant throbbing pain, visible blue lump not spasm-related
- Anal abscess: Constant severe pain with swelling and fever – this is a surgical emergency. For full management options, see anal fistula treatment in Dubai.
- Proctalgia fugax: Sudden severe rectal pain with no visible cause cramp of the levator ani muscle
- Levator ani syndrome: Chronic dull aching pain high in the rectum
Need expert treatment for hemorrhoids, anal fissure, or anal fistula? Book a consultation with Dr. Antonio Privitera in Dubai or Abu Dhabi.
📱 WhatsApp: +971 55 318 8469
📞 Phone: +971 55 318 8469
AUTHOR AUTHORITY BLOCK
Fellowship-trained at Mayo Clinic (USA) and the Royal College of Surgeons (UK). Member of the Royal College of Surgeons of Edinburgh. Certified in General Surgery by the Italian Medical Council.
About the Author
