
Gallbladder Stones (Gallstones)
Gallbladder disease and Gallstones
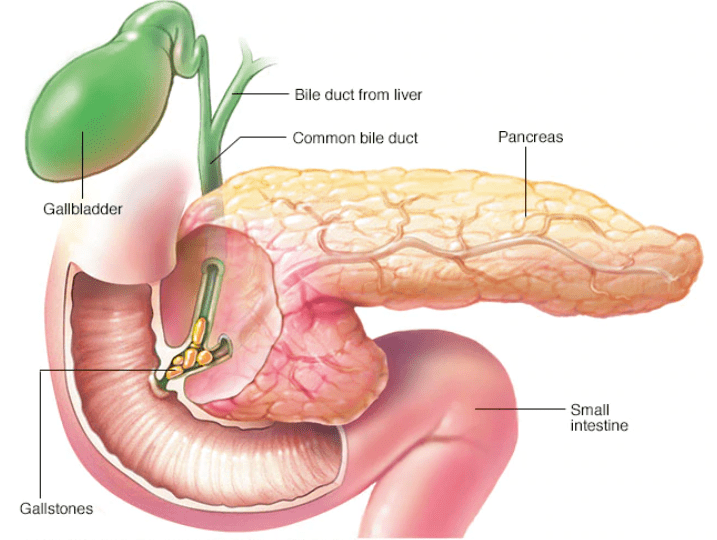
Gallbladder pathology mainly includes gallbladder stones, dysmotility, and rarely neoplasm. The gallbladder is a small gastrointestinal organ that is situated in the right upper quadrant of the abdominal cavity and it is attached to the undersurface of the liver. The main function of the gallbladder is to concentrate and store the bile that is produced by the liver and release it during digestion. Inflammation of the gallbladder usually occurs in the setting of gallbladder stones but may present independently under certain conditions. Gallbladder obstruction caused by stones may lead to biliary colic, overdistension of the gallbladder (hydrops), abscess formation (empyema), and inflammation leading to ischemia, gangrene, and perforation. A gallbladder stone may migrate into the common bile duct and cause obstruction leading to obstructive jaundice, cholangitis, and pancreatitis.
Gallbladder disease is very common and about 20 million adults are affected in the United States. Women are more commonly affected than men, and the prevalence in Mexican-American women reaches 26%. The overall cost of gallbladder diseases in the USA has been estimated to be over 6 billion dollars.
Gallbladder Stone Disease
Gallstones are common in the general population with 10%-20% of adults being affected. Risk factors for cholesterol gallstones include older age, obesity, high fat and low fiber diet, female gender, native American and Mexican-American descent, family history of gallstones, pregnancy, rapid weight loss, low physical activity. The higher incidence in women is likely related to the increased cholesterol level in the bile and the reduced gallbladder contractility induced by estrogens. Gallstones are uncommon in children unless they are affected by certain diseases, in particular hemolytic anemias.
Each year in the USA 500,000 cholecystectomies are performed for symptomatic gallstone disease. Although removal of the gallbladder (cholecystectomy) is a relatively safe procedure, several hundreds of deaths are reported every year in the United States. Around 7,000 cases of mortality every year are related to complications of gallstones, in particular pancreatitis.
01. Pigment Stones
02. Mixed Stones
03. Cholesterol Stones
Types of Gallbladder Stones
There are three main categories of gallstones: cholesterol stones, pigment stones, and mixed stones. About 90% of stones are made of cholesterol and are associated with the risk factors listed above.
- Pigment Stones are small, dark, multiple, and consist mainly of bilirubin and calcium salts. They are more commonly found in people with cirrhosis, infection of the bile ducts, and in patients with hemolytic anemia. Their cholesterol content is <20%.
- Mixed Stones are brown in color and have a cholesterol content between 20-80%. Other components include calcium carbonate, palmitate phosphate, and bile pigments.
- Cholesterol Stones (>80% cholesterol content) have usually a yellow color and form when the bile becomes supersaturated with cholesterol as a result of an increase of its output, reduced production of bile acids, increased mucin secretion, and low gallbladder motility.
Symptoms of Gallbladder Stones
01. Nuclear Medicine Scan
02. Computerized Tomography Scan
03. Endoscopic Retrograde Cholangiopancreatography (ERCP)
04. Magnetic Resonance Cholangiopancreatography (MRCP)
05. X-Rays
06. Ultrasound Scans
Gallbladder Stone Diagnosis
Gallbladder Stones can be diagnosed in multiple ways. Some are invasive and maybe required during chronic formations.
- Nuclear Medicine Scan: Hydroxyl iminodiacetic acid scan (HIDA scan) is indicated in cases of suspected acute cholecystitis in the setting of a negative ultrasound scan. Tc 99m is injected intravenously and it is excreted in the biliary system. If filling of the gallbladder is absent, this is highly suggestive of functional or mechanical obstruction. Injection of cholecystokinin-CCK can also be carried out to measure the ejection fraction of the gallbladder and to reproduce gallbladder symptoms in cases of gallbladder dysfunction.
- Computerized Tomography Scan: Acute gallbladder pathology, gallstones, polyps, can be diagnosed on a CT scan. However, this is not the first imaging modality for gallbladder pathology unless is performed in the workup of gallbladder cancer. The scan is most often performed in the emergency setting when the diagnosis of abdominal pathology is unclear. CT scan has a lower sensitivity than ultrasound scan for the detection of gallstones.
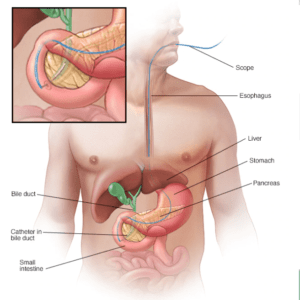
- Endoscopic Retrograde cholangiopancreatography (ERCP): This procedure is performed after reaching the second portion of the duodenum with an endoscope. The papilla of Vater is cannulated and iodinated contrast is injected to visualize the anatomy of the bile ducts. Impacted stones can be removed. Strictures can be treated with sphincterotomy and insertion of stents. Cytology and biopsies can be obtained.
- Magnetic Resonance Cholangiopancreatography (MRCP): This is an MRI examination that provides a detailed assessment of the gallbladder, bile ducts, and pancreas. It is particularly useful in the assessment of bile duct obstruction by stones, strictures, or neoplasms.
- Plain X-ray films: Although plain X-rays have limited value in the diagnosis of gallstones, these may be apparent in 10% of cases due to their calcium content.
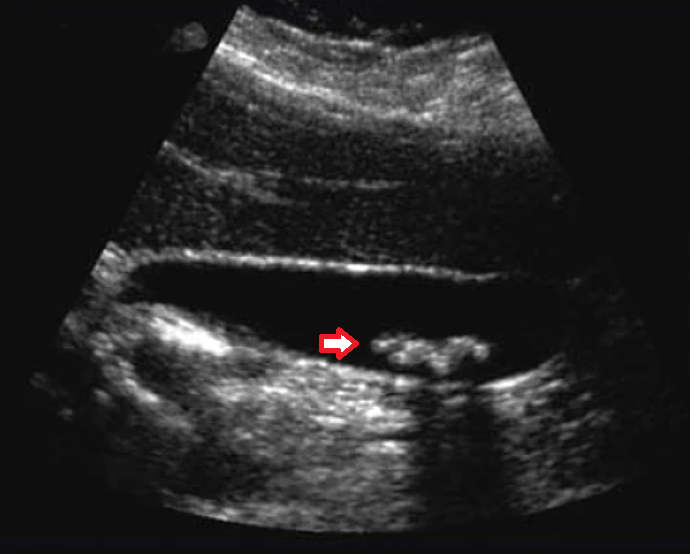
- Ultrasound Scan: The sonographic examination is the gold standard investigation for gallbladder pathology including stones. Signs of acute cholecystitis include wall thickening >5mm, presence of pericholecystic fluid, distension of the gallbladder >5 cm, and sonographic Murphy’s sign positive. The presence of more than one sign increases the accuracy of diagnosis. Gallstones appear echogenic on ultrasound, cast an acoustic shadow, and move with changes in position. An ultrasound scan may also show associated hepatic abscesses or other liver pathology. Assessment of the common bile duct is pivotal and dilatation of this suggests obstruction and stone at this level may be noted.
Gallstones Treatment (Gallbladder Stone Removal)
If gallstones are an incidental finding and do not cause any symptoms, no gallstones treatment is indicated. The old assumption that untreated gallstones may induce gallbladder cancer has no scientific evidence. As gallstones have a high prevalence in the population, it is not surprising that patients with rare gallbladder cancer have gallstones as well. In patients who are symptomatic or in case of emergency, the mainstay of treatment is surgery of gallbladder with stones removal. Medical management (oral dissolution therapy) is often unsuccessful and only indicated in the elective setting when symptomatic patients are unwilling or unfit to undergo gallbladder surgery. With regards to gallbladder stone removal, this is only possible with the removal of the whole gallbladder containing the stones as the gallbladder is the factory of stones. The following points are key gallstones treatments for gallbladder stone removal.
Laparoscopic cholecystectomy
Laparoscopic cholecystectomy has become the gold standard of gallbladder stones removal treatment. Laparoscopy allows for reduced postoperative pain, short hospital stay, faster return to everyday activities, and better cosmesis. More and more laparoscopic cholecystectomies are performed as day cases with the patient being discharged on the same day. In the standard laparoscopic cholecystectomy, four ports are introduced: one for the camera, two working ports, and one for gallbladder retraction. In the case of the very inflamed and overdistended gallbladder, the fluid content can be aspirated before commencing dissection allowing for better handling. The identification of Calot’s triangle formed by the common hepatic duct, cystic duct, and liver, is paramount. This a crucial step to avoid injury to the main bile duct. The cystic artery and duct are carefully dissected, clipped, and divided. The gallbladder is dissected off the liver bed with diathermy. Attention should be paid to the possible presence of accessory bile ducts that must also be secured. The gallbladder with the stones is then placed in an Endobag to avoid spillage, and retrieved from either the umbilical or epigastric port. Accurate hemostasis must be achieved and a drain may be left in the subhepatic space if needed. If in doubt about the anatomy, an intraoperative cholangiogram can be obtained to delineate the anatomy and also to rule out obstruction of the common bile duct. However, common bile duct exploration is rarely performed today. If an obstruction is suspected, the patient should undergo ERCP prior to gallbladder removal and gallbladder stones removal.
Open cholecystectomy
A laparoscopic gallstones treatment approach is the preferred approach for gallbladder and stones removal, however, there are certain circumstances when an open approach is considered: difficulty encountered during laparoscopy with the need for conversion to open surgery; in cases where cholecystectomy is performed together with other procedure carried out with an open approach; in cases of extensive adhesions in patients with previous laparotomies; in the third trimester of pregnancy for technical difficulties to achieve an adequate pneumoperitoneum and handling of laparoscopic instruments.
Cholecystostomy
In cases of acute cholecystitis with the patient unfit to undergo a surgical procedure, drainage of the gallbladder is carried out with the insertion of a cholecystostomy tube usually under radiological guidance.
FAQs About Gallbladder
Symptomatic gallstones usually require surgical removal. Medications rarely dissolve stones effectively or permanently.
Laparoscopic cholecystectomy is one of the most commonly performed and safest surgeries worldwide with excellent outcomes.
Yes. Most people live completely normal lives after gallbladder removal with only minor dietary adjustments initially.
Most patients return to normal activities within 1-2 weeks after laparoscopic gallbladder surgery.
Gallstones form when bile contains too much cholesterol or bilirubin. Risk factors include obesity, rapid weight loss, and family history.
Gallbladder Stone Removal Surgery in Dubai & Abu Dhabi
Most surgeons carry out gallbladder surgery in Dubai and Abu Dhabi. However, a surgeon with a thorough understanding of the anatomy and extensive laparoscopic experience is of extreme importance to avoid injuring the bile duct and major vascular structures, particularly in the emergency setting when the inflammatory process may make recognition of the anatomy and the dissection very challenging.
Looking for Gallbladder Stone Removal in Dubai & Abu Dhabi?
A proctology service not only for Gallbladder Stone Removal in Dubai and Abu Dhabi but also for many other diseases is currently available at leading hospitals in the region. Dr. Antonio Privitera is offering a free consultation for gallbladder disease treatment in Dubai and Abu Dhabi.
Book an Appointment
