
Endoscopy Procedure and the endoscopist
What is Endoscopy?
Endoscopy is a diagnostic and therapeutic tool that allows to identify abnormalities of the gastrointestinal tract (esophagus, stomach, duodenum, small intestine, colon and rectum). Esophago-gastro-duodenoscopy (commonly called gastroscopy), colonoscopy, small bowel enteroscopy and capsule endoscopy are the procedures usually performed.
Endoscopy of the large bowel (colonoscopy) is often used to screen for colon and rectal cancer, colon and rectal polyps, diverticular disease, inflammatory bowel diseases and to perform interventional procedures. A colonoscope is a long, thin, flexible instrument that provides magnified views of the colon and rectum. In certain circumstances, a flexible sigmoidoscopy that examines only the left side of the colon could be enough (e.g. bleeding on defecation in a young patient). This endoscopy procedure is most commonly performed under sedation in the outpatient setting with minimal discomfort and inconvenience.
.
When Do you need an Endoscopy?
The main indications for colonoscopy are: change in bowel habits with recent onset of diarrhea or constipation, rectal bleeding, anemia, unexplained weight loss, abdominal pain. It is also important as a screening tool in patients above the age of 45 or with a family history of bowel cancer. Endoscopic follow-up is required for patients with previous polyps, hereditary conditions predisposing to bowel cancer (Familial Adenomatous Polyposis – FAP, Hereditary Non Polyposis Colorectal Cancer – HNPCC, previous bowel resection for cancer and chronic inflammatory diseases (Crohn’s disease or Ulcerative colitis).
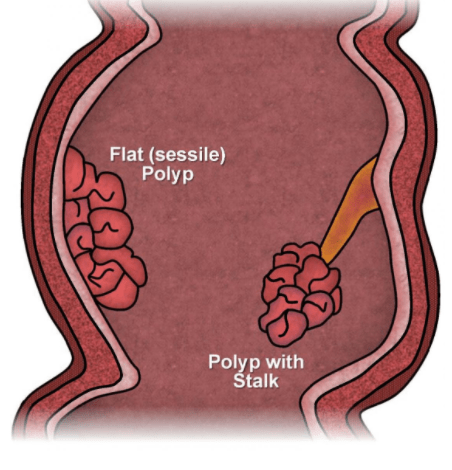
Recommendations for screening differ according to Societies, but it is generally recommended that average-risk patients undergo a colonoscopy > 45 years. However, in patients with a strong family history of bowel cancer or known hereditary bowel cancer syndromes, a shorter follow-up is required. If an adenomatous polyp is found at flexible sigmoidoscopy, a full examination of the colon should be carried out as 40% of the patients will have other polyps. When patients present with symptoms suggesting colorectal cancer or when screening imaging identifies potential tumors, a colonoscopy should be obtained. There is no reported malignancy in polyps < 5mm, but the endoscopist would excise them for the potential of them growing over time.
How is Endoscopy (Colonoscopy) performed?
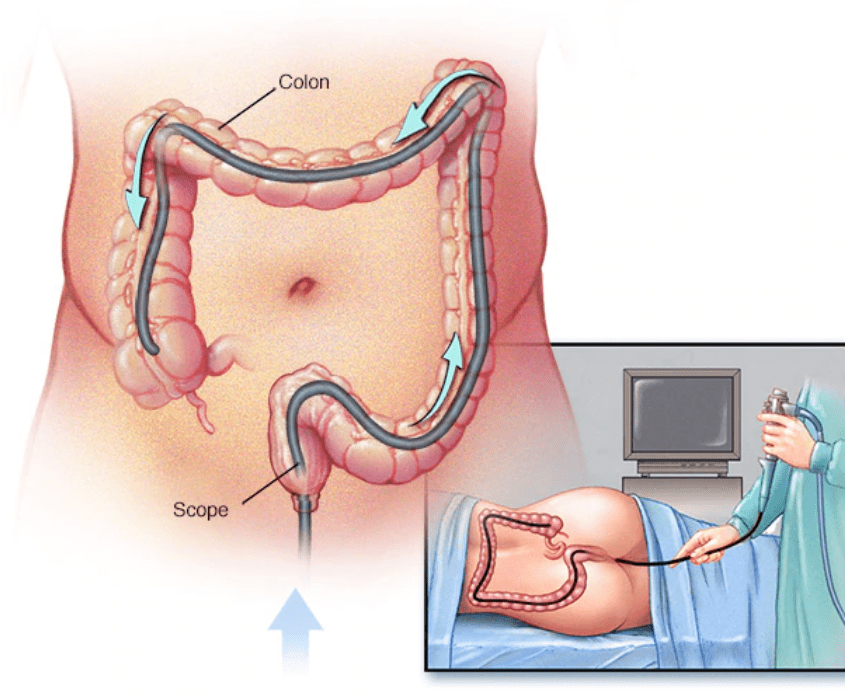
The patient is placed in the left lateral position. A long flexible instrument of the diameter of about 1 cm is used. The tip of the instrument contains a camera, an air/suction/irrigation channel and an operative channel for insertion of biopsy forceps, clip applicator, coagulation devices etc. At the start of the procedure, the tip of the instrument is well lubricated and inserted gently into the anus.
Air inflation will distend the rectum and will show the Valves of Houston that are folds in the rectum that correspond to its curvatures. The passage into the colon is through a segment that is called recto-sigmoid junction. This step can cause particular discomfort due to its acute angulation. The first part of the colon to be examined is the sigmoid. Depending on the length of the sigmoid and its tortuosity, passage of the instrument may be more or less challenging. The ability of the endoscopist is to keep the instrument short by allowing the colon to create a concertina-like shape over it.
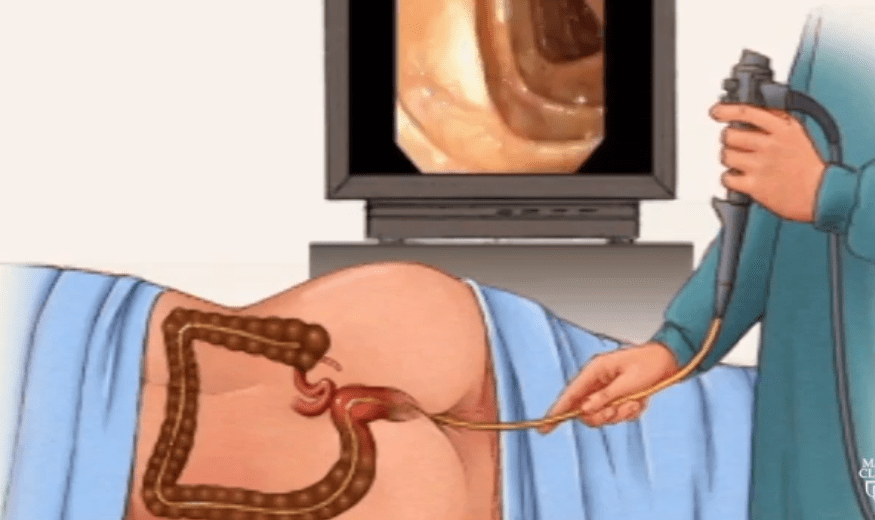
It is pivotal that every part of the colon is examined at 360 degrees not to miss any lesion, especially around turns and angulations where blind spots can be created. Following a short, straight part of the colon (descending colon), the instrument is manipulated through the splenic flexure and then into the transverse colon. At this point, it is best to turn the instrument clockwise and pull back with gentle air suction. This allows to resolve any loops that may have formed in the sigmoid colon. The transverse colon can be tortuous and long depending on the length of its mesentery. Once the hepatic flexure is passed, the instrument will reach the ascending colon and the cecum concluding the examination of the colon.
There are 4 main features that allow to be confident to have reached the cecum: the ileocecal valve, the tridate fold, the appendiceal orifice, and transillumination in the right iliac fossa. Routine intubation of the terminal ileum is recommended. This is particularly important if lesions are suspected in the small bowel (e.g. inflammatory bowel diseases). A biopsy of the ileum is the only 100% proof that the examination has been complete. Photographs are obtained of the main landmarks and of any lesions detected. Withdrawal of the instrument is a very important step. Each segment must be examined carefully as the instrument is pulled back in order to identify any lesions that may have been missed on the way in.
Endoscopy Procedure
Colonoscopy is performed by the endoscopist (gastroenterologist or colorectal surgeon- proctologist). Gastroenterologists and proctologists must work as a team to improve patient’s colorectal diseases management. As a matter of fact, inflammatory bowel diseases are first treated medically by the gastroenterologist and in case of no response or development of complications, the colorectal surgeon is ready to intervene. The gastroenterologist may remove a polyp that turns out to be malignant and refer the patient to the colorectal surgeon for further management. Colonoscopy tests are performed in many hospitals, but an expert endoscopist is needed to improve detection and identification of lesions and reduce complication rate. The colonoscopy procedure is performed as a day case and the patient is discharged as soon as the effect of sedation medications wears off. The cost of colonoscopy in Dubai and Abu Dhabi can be very high. However, Dr. Antonio offers very competitive rates that suit every insurance or cash payers
indications for an emergency colon and Rectal Endoscopy
Lower gastrointestinal bleeding is one of the main indications for emergency colonoscopy. The bleeding point can be identified and therapeutic interventions can be carried out to control the bleeding: injection of epinephrine, diathermy, argon plasma coagulation, clipping, etc. If time allows, a quick bowel preparation can be helpful to improve the endoscopic view. Common causes of lower gastrointestinal bleeding include: diverticular disease, artero-venous malformations, hemorrhoids, tumors, radiation induced proctitis, etc.
In the case of a twist of a segment of colon (volvulus), colonoscopy can be used to derotate and decompress the bowel and straighten the colon allowing for a bridge to definitive surgical treatment. When a tumor is obstructing the lumen of the bowel, colonoscopy together with fluoroscopy allows for an accurate positioning of a stent that may be palliative or a temporary measure until bowel resection. In case of short stricture of benign nature, a balloon dilatation can be carried out.
In case of pseudo-obstruction of the colon (Ogilvie syndrome) characterized by a dilatation of the colon in the absence of a mechanical obstruction, decompression by colonoscopy may avoid ischemia and perforation of the bowel. This should be performed by expert operators and with little insufflation as the risk of perforation is high.
FAQs About Endoscopy
It is very important that the bowel is clean in order to have a clear view and identify the smallest of lesions. Polyethylene glycol (PEG) is a commonly used osmotic laxative that produces watery diarrhea. It also contains electrolytes to replenish losses. Picosulfate is another laxative that together with magnesium citrate produce an effective cleansing. The day before the procedure a fluid diet is followed. Red food or drinks that may be misinterpreted as blood should be avoided.
Conditions that increase the risk of colonic perforation are considered contraindication to colonoscopy. These include: suspicion of bowel perforation, fulminant colitis, toxic megacolon, etc. The procedure is best avoided during pregnancy, although definitive evidence in the literature does not exist.
Although there is a risk of 2-5% of bacteria dislodging into the blood (bacteremia) during the procedure, the risk of this producing complications is extremely low. Therefore, antibiotics are not routinely advised, but they may be considered in select patients (presence of prosthetic valves, previous endocarditis, congenital heart diseases, presence of joint replacements, etc).
Commonly, conscious sedation is administered with intravenous midazolam, fentanyl or pethidine. The patient is still conscious and may be asked to change position to facilitate the progression of the instrument. Sometimes, hand pressure on the abdomen is applied to aid the examination. Some patients prefer to be deeply sedated and have no recollection of the procedure. In this case, the presence of an anesthetist is required.
- Virtual endoscopy: This a high-resolution CT scan performed after introducing air to distend the colon. Smooth-muscle relaxants can be administered. The procedure is less invasive than colonoscopy and accurate in the detection of polyps and tumors and in the assessment of their size, shape and location. Main disadvantages include reduce accuracy to identify small polyps and inability to obtain a biopsy.
- Colon capsule endoscopy: The procedure utilizes a wireless video capsule that is swallowed and provides an assessment of the colon without need of sedation and colon air insufflation. Technical features still must be improved to allow the procedure to have the same accuracy of traditional endoscopy and have widespread use.
Need an Endoscopist in Dubai & Abu Dhabi?
A proctology service in Dubai and Abu Dhabi, not only for Colonoscopy but also for many other diseases, is currently available in both cities
Book an Appointment
