
Hemorrhoids or Piles Treatment
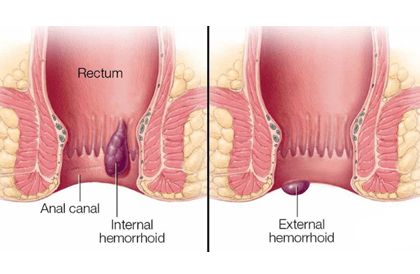
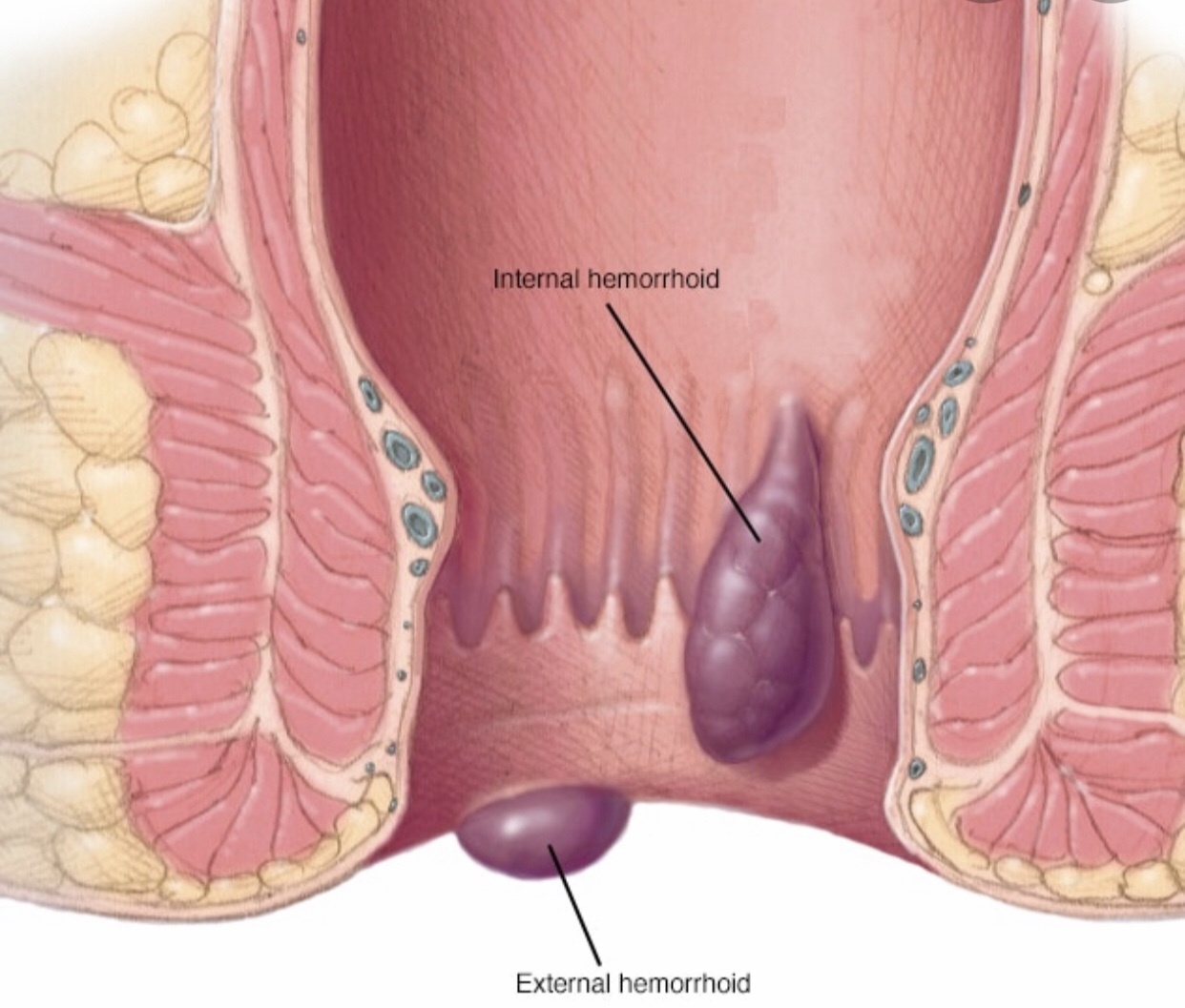
The term ‘hemorrhoid or piles’ comes from the Greek and means ‘flowing blood’ and this is something not normal. Despite this, many specialized books erroneously refer to hemorrhoids as a normal part of the anatomy and this is far from the truth. Haemorrhoids are a disease of the anal cushions that consist of clusters of connective tissue, smooth muscle, and vascular structures covered by mucosa and arranged in the typically described position of 3,7,11 o’clock in the anal canal. Their function is to contribute to the anal continence at rest. Internal hemorrhoids are situated above the dentate line and are supplied by the internal hemorrhoidal plexus that is a dependence of the superior rectal vessels. External hemorrhoids are situated below the dentate line and are supplied by the external hemorrhoidal plexus that is formed by the inferior rectal vessels. These two plexuses have some communications (A-V shunts) that are usually closed in normal circumstances. In haemorrhoidal disease, these shunts sometimes open up and an internal hemorrhoid is seen to continue with external hemorrhoids without distinct separation between them. We refer to this situation as ‘internal-external hemorrhoid’. Internal hemorrhoids have visceral innervation while external hemorrhoids have somatic innervation. Dr. Antonio Privitera is a world-renowned surgeon and is a piles or hemorrhoids doctors in Dubai, Abu Dhabi and Al Ain.
About Hemorrhoids or Piles
The prevalence of haemorrhoids in the United States of America is about 4-8%. Hemorrhoids have been reported in up to 38% of screening colonoscopies, however, only 44% are symptomatic. Age > 45 and obesity are the main risk factors.
Traditionally, internal hemorrhoids have been divided into 4 grades. Grade I hemorrhoids are seen on anoscopy as a bulge in the anal canal but no prolapse. Grade II protrude on straining but spontaneously reduce. Grade III hemorrhoids prolapsed and require manual reduction. Grade IV hemorrhoids are characterized by permanently prolapsed hemorrhoids outside the anus with the frequent presence of fibrotic changes and skin tags.a
Causes of Hemorrhoids or Piles
There are a few theories that have tried to explain the origin of hemorrhoids. A diet poor in fibers leading to constipation and excessive straining on defecation has for long been considered the main risk factor. This could explain the higher incidence of the disease in the Western countries compared for example to the African countries. Posture in the course of defecation seems to also have an important role. In societies that have followed western habits, the sitting position during defecation produces a more acute anorectal angle with consequent greater strain on the anal canal. The straining would lead to stretching and structural changes in the anal cushions with a reduction of the venous outflow and opening of artero-venous anastomoses creating a high venous pressure system. A general laxity of tissues contributes to this mechanism. Hemorrhoids have been described in patients with Ehlers-Danlos syndrome suggesting that a collagen abnormality can be a predisposing factor. An increase in matrix metalloproteinases that regulate extracellular proteins and remodeling of tissues has been observed in hemorrhoids sufferers.
Other studies have found an association with diarrhea instead of constipation. Diarrhea itself puts a strain on the anal canal as the patient will need to empty his bowels several times a day.
Symptoms of Hemorrhoids or Piles
Internal haemorrhoids most often present with painless rectal bleeding and/or prolapse. Prolapse can produce soiling, mucous discharge, and skin irritation. Painful internal hemorrhoids are usually the result of thrombosis, incarceration, and strangulation. Complicated external hemorrhoids are often exquisitely painful due to their somatic innervation. This may happen in the case of hematoma or thrombosis within hemorrhoids. When the clot is reabsorbed, the inflammatory reaction and healing may leave skin tags. These can become irritated or create problems with hygiene.
Symptoms of hemorrhoids are often self-limiting and respond well to conservative measures: dietary changes with an increase in fluid and fiber intake, laxatives, regular exercise, avoidance of constipation and straining, modifications of toilet habits.
Diagnosis of Hemorrhoids or Piles
The diagnosis of hemorrhoids is based on clinical history and examination. It is pivotal not to attribute rectal bleeding to hemorrhoidal disease until a full workup has been carried out. Anoscopy and rigid proctoscopy can be easily performed in the clinic. Flexible sigmoidoscopy or full colonoscopy can be carried out on a case by case basis.
Treatments for Hemorrhoids or Piles
- Hemorrhoids treatment with fiber supplementation has been shown to decrease rectal bleeding by 50%, however, it seems to have little impact on prolapse, pain, and itching. There is no evidence to support the benefit of steroid and local anesthetic topical over-the-counter medications.
- Phlebotonics are a class of medications that have the property to increase venous tone, stabilize the permeability of capillaries, and improve lymphatic drainage. A Cochrane review has shown that hemorrhoids treatment with phlebotomids compared to control groups improve bleeding, itching, discharge, and leakage. Mild gastrointestinal side effects are reported.
Methods of Hemorrhoids or Piles Surgery
Surgical hemorrhoids treatment includes office-based procedures that do not require anesthesia and others that are performed under local, regional, spinal, or general anesthesia. The choice of treatment depends on the Grade of hemorrhoids and the associated symptoms. Painless hemorrhoids treatment can be achieved with the new techniques that are associated with only mild discomfort.
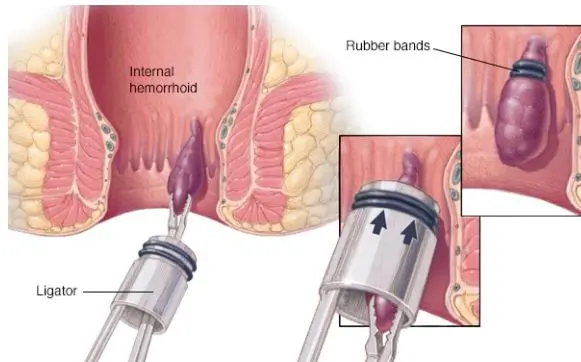
Rubber band Ligation
Rubber band ligation is the most commonly performed procedure in the outpatient department for Grade I and Grade II hemorrhoids or piles. It can also be used for Grade III, but the risk of recurrence is high, and usually, more sessions are required. Suction devices are most often used.
The band is generally applied just above internal hemorrhoids to interrupt the blood supply and produce ischemia, sloughing, followed by ulceration and healing over a few weeks. A dull discomfort is usually felt as the band is placed above the dentate line where there is visceral innervation. Complications include severe pain (related to improper band positioning or thrombosis), urinary retention, delayed rectal bleeding, and rarely sepsis. The overall success rate is about 70%.
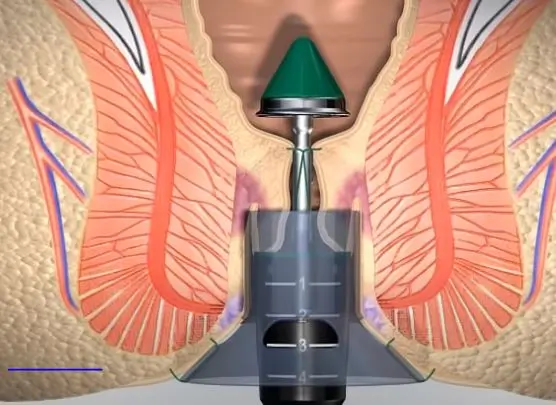
Stapled hemorrhoidopexy
Stapled hemorrhoidopexy is based on the concept of removing part of the lower rectal mucosa to lift the hemorrhoids and cut off the blood supply. The resulting staple line must be away from the dentate line to avoid severe postoperative pain. Usually, this is around 4 cm from the anal verge. Circumferential Grade III hemorrhoids are the ideal indication for this kind of procedure that has the advantage of reduced postoperative pain.
However, surgeons must have sufficient training on the stapling device to avoid rare but possibly described specific complications including recto-vaginal fistula, stenosis, perforation, and anal sphincter injury. Studies have shown that long-term results are better with excisional hemorrhoidectomy than hemorrhoidopexy.

Doppler-Guided hemorrhoidal artery ligation
Doppler-guided hemorrhoidal artery ligation uses a special proctoscope with a Doppler probe that identifies and allows to tie the branches of the superior rectal artery that supply the hemorrhoids. Also, a mucopexy is performed to plicate the associated rectal mucosal prolapse.
Hemorrhoidectomy
Hemorrhoidectomy involves the surgical excision of hemorrhoids and it is associated with the best long-term results with the downside of an increased number of complications and pain. An elliptical incision is made in the skin close to the anal verge and the hemorrhoid column is dissected off the internal sphincter and its pedicle divided. This is a critical step of the procedure as an injury to the internal sphincter may lead to incontinence. Also, it is mandatory to preserve bridges of intact mucosa to prevent anal stenosis. The wound defect can be left open to heal (Milligan-Morgan technique) or closed with sutures (Ferguson technique). Postoperative pain can be severe in the first few days and this is the reason why numerous mini-invasive techniques have been developed.
Laser Hemorrhoids or Piles Treatment
Laser hemorrhoid treatment is a technique that produces shrinkage of the hemorrhoids through the insertion of a laser probe into the hemorrhoid tissue. Attention should be taken not to direct the probe towards the internal anal sphincter and to apply ice after each application to reduce heat damage. A mucopexy is also performed. Pain is less than traditional hemorrhoidectomy.
Sclerotherapy
Infrared Coagulation
Emergency Hemorrhoids or Piles Surgery
Emergency surgery for internal hemorrhoids should only be performed in case of strangulation or inability to reduce incarcerated hemorrhoids caused by prolapse with anal sphincter spasm. Most of the time emergency reduction can be obtained after the application of sugar or salt to reduce edema. Thrombosed external hemorrhoids are usually severely painful in the first 48-72 hours. Subsequently, the pain subsides as the hematoma is reabsorbed. Conservative measures with fiber supplements, laxatives, and local anesthetic are usually adopted. Unroofing of external hemorrhoids and evacuation of the clot or full excision is indicated in cases of severe pain non-responding to analgesia and case of recurrent symptoms.
Hemorrhoids or Piles Doctor in Dubai, Abu Dhabi and Al Ain
Most surgeons and some physicians commonly perform hemorrhoids treatment in Dubai and Abu Dhabi. However, patients must be aware that the best results of hemorrhoids treatment in Dubai and Abu Dhabi are achieved by colorectal surgeons who have a full understanding of the anatomy, and they are skilled with the various techniques and able to tailor treatment to each individual. Problems that may arise from improper treatment include fecal incontinence and severe long-lasting pain that severely impair the quality of life. People would generally search on internet search engines for a “Hemorrhoids or Piles Doctors in Dubai and Abu Dhabi” and be confused by the many clinics and hospitals offering a vast array of options. A hemorrhoids treatment doctor in Dubai and Abu Dhabi should be a colorectal surgeon with reputable fellowship training, a member of colorectal societies, and with a dedicated history of practice in the field. A hemorrhoids treatment doctor in Dubai and Abu Dhabi should well know when not to operate and how to best resolve the patient’s symptoms. In the absence of prolapse, a hemorrhoids doctor should not perform a stapled hemorrhoidopexy. Any hemorrhoids treatment doctor in Dubai and Abu Dhabi should know that there is no point in treating surgically thrombosed external hemorrhoids after 72 hours. The hemorrhoids treatment doctor in Dubai, Abu Dhabi and Al Ain should consider a formal hemorrhoidectomy for Grade IV hemorrhoids, especially when fibrotic changes and multiple skin tags are present.
Haemorrhoids or Piles FAQs
Do I need treatment, or do haemorrhoids (piles) typically resolve on their own?
Hemorrhoids, or piles, can sometimes resolve on their own, especially if they are small and not causing significant symptoms. However, this varies widely among individuals. For persistent or worsening symptoms such as pain, itching, or bleeding, treatment is often recommended to alleviate discomfort and promote healing. Conservative measures such as dietary modifications to increase fiber intake, topical treatments (creams, ointments), and sitz baths can help manage symptoms effectively. In more severe cases, procedures like rubber band ligation, sclerotherapy, or surgery may be necessary to fully resolve hemorrhoids. It’s advisable to consult with a healthcare provider to determine the most appropriate treatment based on the severity and persistence of your symptoms.
How does exercise benefit my hemorrhoids?
Exercise benefits hemorrhoids in several ways. Regular physical activity improves blood circulation throughout the body, including the veins in the rectal area where hemorrhoids develop. Improved blood flow helps reduce swelling and inflammation of hemorrhoidal veins, which can alleviate symptoms such as pain, itching, and discomfort. Additionally, exercise promotes regular bowel movements by stimulating the muscles of the colon and rectum, which reduces the strain and pressure on hemorrhoids during defecation. Exercises that strengthen the pelvic floor muscles, such as Kegel exercises, can further support bowel function and reduce the risk of hemorrhoid formation or exacerbation. Overall, incorporating moderate aerobic activities like walking, swimming, or cycling into your routine can contribute to better digestive health and help manage hemorrhoid symptoms effectively.
Is there a definitive way to confirm if I have hemorrhoids (piles)?
Yes, there is a definitive way to confirm if you have hemorrhoids (piles). A healthcare provider can typically diagnose hemorrhoids through a combination of medical history and physical examination. During the examination, they may visually inspect the anal area for swollen blood vessels or perform a digital rectal examination to feel for internal hemorrhoids. In some cases, additional diagnostic procedures such as anoscopy or sigmoidoscopy may be recommended to further evaluate the extent and location of hemorrhoids. These tests allow the healthcare provider to confirm the presence of hemorrhoids and rule out other conditions with similar symptoms, ensuring accurate diagnosis and appropriate treatment.
I've had haemorrhoids in the past. Should I consider taking fiber supplements?
If you’ve had hemorrhoids in the past, considering fiber supplements may be beneficial. Fiber supplements, such as psyllium husk or methylcellulose, can help soften stools and make them easier to pass. This reduces the need for straining during bowel movements, which is a common trigger for hemorrhoids. Increasing fiber intake through supplements or dietary sources like fruits, vegetables, and whole grains can promote regular bowel movements and prevent constipation, thereby reducing the risk of hemorrhoid recurrence. It’s important to consult with a healthcare provider before starting fiber supplements to determine the appropriate type and dosage based on your individual needs and medical history.
Can surgery for haemorrhoids (piles) be avoided?
In many cases, surgery for hemorrhoids (piles) can be avoided through conservative treatments and lifestyle modifications. Initial management typically includes dietary changes to increase fiber intake, which helps soften stools and reduce straining during bowel movements. Over-the-counter medications such as topical creams or suppositories can provide relief from symptoms like pain and itching. Additionally, adopting good bowel habits, such as avoiding prolonged sitting and staying hydrated, can help alleviate symptoms and prevent hemorrhoid progression. Non-surgical procedures like rubber band ligation, sclerotherapy, or infrared coagulation are effective alternatives for treating persistent hemorrhoids without the need for surgery. However, for severe or recurrent hemorrhoids that do not respond to conservative measures, surgical intervention may be necessary. Consulting with a healthcare provider is crucial to determine the most appropriate treatment approach based on the severity and persistence of your symptoms.
Are ahemorrhoids (piles) potentially dangerous?
Hemorrhoids (piles) themselves are generally not considered dangerous, but they can cause significant discomfort and affect quality of life. Common symptoms include pain, itching, swelling, and bleeding during bowel movements. In some cases, hemorrhoids may become thrombosed (develop blood clots) or prolapsed (protrude outside the anus), which can lead to complications requiring medical intervention. Severe bleeding or persistent symptoms despite conservative treatment may indicate the need for further evaluation by a healthcare provider. While hemorrhoids are not life-threatening, complications such as severe bleeding or infection can occur, underscoring the importance of seeking medical attention if you have concerns or experience unusual symptoms associated with hemorrhoids.
Which treatment is best for hemorrhoids?
The best treatment for hemorrhoids depends on the severity of the condition and individual factors. Mild cases often respond well to conservative measures such as dietary changes to increase fiber intake, topical treatments (creams, ointments), and sitz baths. For more persistent or severe hemorrhoids, minimally invasive procedures like rubber band ligation, sclerotherapy, or infrared coagulation are effective options. These procedures help shrink hemorrhoidal tissue and alleviate symptoms without the need for surgery. In cases where hemorrhoids are large or do not respond to other treatments, surgical options such as hemorrhoidectomy may be considered. The choice of treatment should be tailored to each patient’s specific symptoms, preferences, and medical history, so consulting with a healthcare provider is essential to determine the most suitable approach.
Does insurance cover piles treatment in Dubai?
Insurance coverage for piles treatment in Dubai can vary depending on the insurance policy and provider. In general, many health insurance plans in Dubai cover treatments for medical conditions, including hemorrhoids (piles), especially if deemed medically necessary by a healthcare provider. However, coverage specifics, such as the types of treatments included, co-payments, deductibles, and network providers, may differ between insurance plans. It is advisable to check with your insurance provider directly to understand the extent of coverage for piles treatment, including consultations, procedures, medications, and any associated costs. This ensures clarity on what expenses are covered and any potential out-of-pocket costs you may incur.
Is it bad to leave haemorrhoids untreated?
Leaving haemorrhoids untreated can lead to worsening symptoms and potential complications. Hemorrhoids can cause persistent pain, itching, and discomfort, affecting daily life and quality of life. Without treatment, hemorrhoids may become more swollen, prolapsed (protrude outside the anus), or thrombosed (develop blood clots), which can increase pain and require more invasive treatment. Persistent bleeding from hemorrhoids can also lead to anemia over time if left untreated. It’s important to seek medical advice if you have symptoms of hemorrhoids to receive appropriate treatment and prevent complications. Early intervention with conservative measures or medical treatments can effectively manage symptoms and promote healing, reducing the need for more invasive procedures later on.
Looking for Hemorrhoids or Piles Doctors in Dubai, Abu Dhabi and Al Ain?
A proctology service not only for piles & hemorrhoids treatment but also for many other diseases is currently operating in Dubai London Hospital, Aster Hospital, American Hospital. Currently, Dr. Antonio Privitera is offering a free consultation for hemorrhoids or piles treatment in the same hospital in Dubai, Abu Dhabi and Al Ain.