
Rectal Prolapse
What is a Rectal Prolapse?
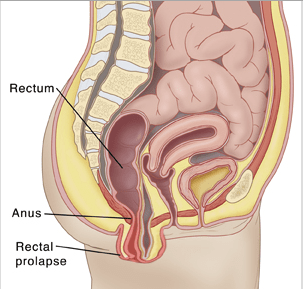
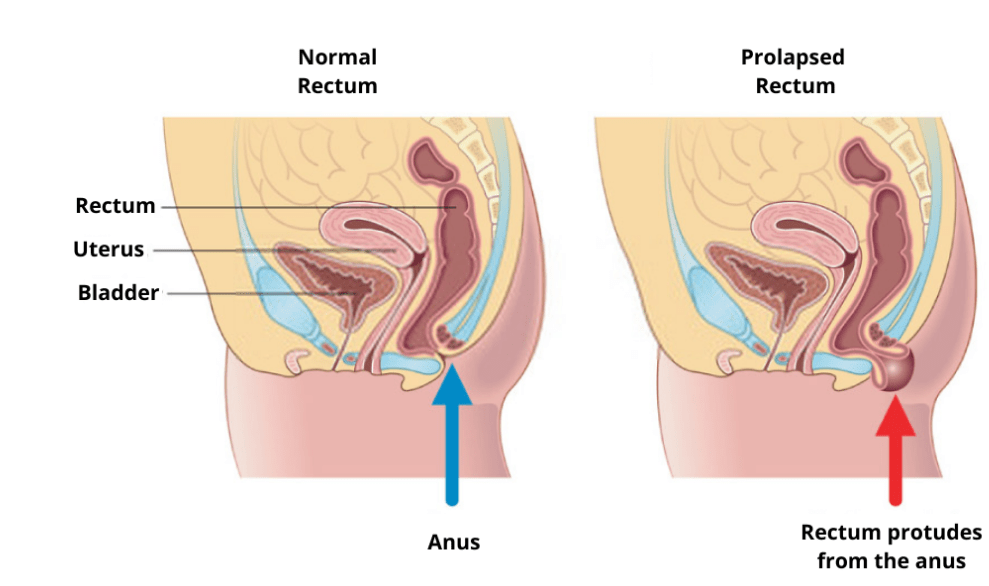
Rectal prolapse is a protrusion of the rectal wall outside the anus. This can involve only part of the rectal wall (mucosal prolapse) or all the layers of the bowel wall (full-thickness prolapse). When the prolapse is only internal and does not prolapse out of the anus is referred to as ‘internal prolapse’ that is a common cause of obstructive defecation.
What are the causes of a Rectal Prolapse?
Anatomical abnormalities predispose to the formation of rectal prolapse: diastasis of the levator ani muscle plate, a deep recto-vaginal or recto-vesical pouch of Douglas, an excessively long sigmoid colon, a weak anal sphincter complex, a patulous anal sphincter, and abnormalities of the rectal attachments to the sacrum. Rectal prolapse affects 0.5% of the population in particular women and the elderly. The incidence in women above 50 years of age is 6 times higher than in men. Although it is generally thought that rectal prolapse is prevalent in women with multiple pregnancies, 1/3 of affected women are nulliparous. Interestingly, the disease seems to affect men at a younger age than women. Risk factors also include psychiatric history with the use of more than one medication, autism, and developmental disorders.
Rectal Prolapse Symptoms
Despite rectal prolapse being a benign condition, symptoms may greatly affect everyday life. These include pain due to the prolapsing tissue that may get incarcerated or strangulated, rectal discharge of mucous or blood, fecal incontinence, or constipation. Fecal incontinence is reported by 50-75% of patients and is related to the prolapse keeping the anus open; the chronic stretch of the anal muscle that may lead to weakness and structural abnormalities; the continuous activation of the recto-anal inhibitory reflex; pudendal neuropathy that is observed in 50% of cases. Constipation is reported in 25-50% of cases. This is related to blockage of the anus by the prolapse that is exacerbated by straining and pelvic floor dysmotility.
Rectal Prolapse Diagnosis
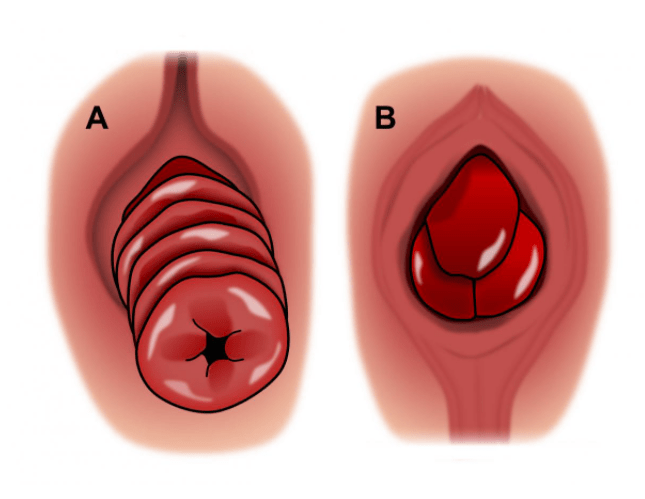
The initial assessment of the patients should include a thorough clinical history and examination. Concomitant prolapse of other organs is present in a third of cases and should also be investigated as it may require a multidisciplinary approach (vaginal and/or uterine prolapse, urinary symptoms such as incontinence). The examination would normally start in the left lateral position that may reveal a patulous anus, an obvious protruding prolapse, pelvic descent on straining, etc. Anal and rectal examination in the clinic with an anoscope and rigid proctoscope is essential to rule out other diseases. It is important to distinguish between a full rectal prolapse that will have concentric folds from a mucosal rectal prolapse that presents radial invaginations. Sometimes, the prolapse is not evident on clinical examination and it is important in these cases to ask the patient to strain in the sitting position or squatting. An enema can be helpful in these circumstances. The patient may bring photographic evidence of the prolapse. A defecography under fluoroscopy or better an MRI defecography are a very important tools in the diagnosis of rectal prolapse and to plan surgical management. A full colonoscopy may be considered in some cases.
Rectal Prolapse Conservative Treatment
Despite the only treatment of rectal prolapse being surgery, some of the symptoms may be alleviated by medical therapy and behavioral modifications. Dietary modification and the use of fiber supplements or laxatives may be helpful in patients with constipation. Antimotility drugs may be beneficial in cases of fecal incontinence. Patients who are fit for surgery should be advised to undergo surgical management to avoid possible risks of incarceration/strangulation, irreversible fecal incontinence, and a higher risk of recurrence after surgery, especially if untreated for > 4 years.
Pelvic Organ Prolapse & Prolapsed Uterus Treatment
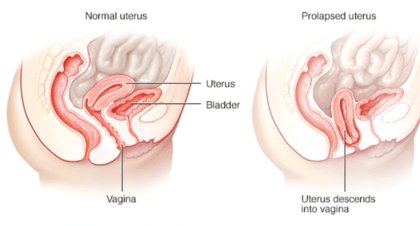
Pelvic organ prolapse (POP) is a descent of the organs in the pelvis from their normal position and it is caused by loss of structural support. This may lead to prolapse of the uterus, vaginal prolapse, bladder prolapse, urethral prolapse, and rectal prolapse. In uterovaginal prolapse, the uterus, cervix, and upper vagina are involved. An abnormality in the supporting system of the pelvic organs is the basic pathophysiological mechanism in the formation of prolapse. Muscles, ligaments, and soft tissues may be damaged, stretched, or weakened with aging. Risk factors include pregnancy with vaginal delivery, hysterectomy, pelvic surgery, menopause, obesity, chronic constipation, repeated heavy lifting, genetic predisposition, and connective tissue disorders.
Symptoms of pelvic organ prolapse include pelvic discomfort, bulging of organs through the vaginal opening, urinary incontinence, and sexual difficulties. In the case of uterine prolapse, symptoms severity is usually related to the uterine prolapse stages: Stage 1, uterine descent reaches the upper third of the vagina; Stage 2, the prolapsed cervix reaches the introitus; Stage 3, the uterus protrudes out of the vagina.
Prolapsed uterus treatment is not usually needed in milder forms of the disease. Several non-surgical options can be adopted in the treatment of a prolapsed uterus. These include: pelvic floor exercises, losing weight, avoiding heavy lifting, hormone (estrogens) treatment, or wearing a pessary. In severe cases or inability to control symptoms prolapsed uterus treatment with surgery is considered. Main surgical options include hysterectomy with sacrocolpopexy, hysteropexy, and Manchester procedure.
Rectal Prolapse Surgery
Several techniques have been described for the surgical treatment of rectal prolapse. Anal encirclement, Delorme’s procedure (mucosal resection and muscle plication), Altemeier’s procedure (perineal procto-sigmoidectomy), Stapled Trans-Anal Rectal Resection -STARR, suture rectopexy, resection rectopexy, anterior/ventral or posterior rectopexy with mesh, etc. Abdominal approaches can be performed with minimally invasive surgery (laparoscopic or robotic) reducing the hospital stay and allowing for a fast return to normal activities. It is important to tailor the treatment to the individual patient and to discuss the pros and cons of each procedure. There are two main groups of surgical approaches: abdominal or perineal. Although traditionally it was thought that abdominal operations have a higher success rate, this has recently been questioned as the outcomes seem to be similar.

Posterior Rectopexy
Mobilization of the rectum posteriorly down to the pelvic floor and suturing the rectum with nonabsorbable materials to the sacral promontory are the two important steps of this procedure. The addition of a mesh has been shown not to decrease the recurrence rate and to increase the rate of complications. This technique, especially when combined with the division of the lateral rectal stalks, is reported to worsen constipation. Therefore, in inpatient complaining of preoperative constipation, a sigmoid resection is recommended at the same time.
Anterior (Ventral) Rectopexy
Ventral rectopexy with the use of mesh has gained popularity in the last few years, especially in patients with pre-existing constipation and enterocele. Posterior rectal dissection that is thought to worsen constipation by disruption of the autonomic innervation, is avoided. The rectum is anteriorly freed from the vagina or prostate down to the perineal body. A mesh is sutured to the anterior rectal wall and the sacral promontory thus suspending the rectum. Ventral rectopexy has been shown to improve constipation. Recurrence rates of <10 % have been reported.
Delorme’s Procedure
In case of short rectal prolapse (<5 cm) a mucosal sleeve resection can be performed. The prolapse is fully pulled out and a circular incision is performed 2 cm above the dentate line. The mucosa is gently dissected off the muscular layer for the whole length of the prolapse. A series of absorbable sutures are used to plicate the bowel wall muscle and finally, the mucosa is approximated with interrupted sutures. Recurrences of 10-15 % have been reported. Recent randomized trials have shown that outcomes of this procedure are comparable to other perineal or abdominal approaches.
Altmeyer’s Procedure
Perianal proctosigmoidectomy involves a transanal resection with colo-anal anastomosis. Complications are lower, and the hospital stay is shorter when compared to abdominal surgery. However, a high recurrence rate of up to 30 % has been reported. The addition of keratoplasty seems to reduce recurrence rates to <10 %. A modification of the technique reported by Prof. Antonio Privitera is the addition of laparoscopy to make sure that the redundant bowel is completely excised.
Transanal resection of rectal prolapse using a stapling device is safe and effective with low recurrence rates. The use of staplers up to 36 mm has facilitated the procedure. A purse-string or parachuting technique is used and a full circular full-thickness resection is performed. It is very important to secure with sutures any bleeding points in the staple line. Particular attention is to be paid in females in order not to include the vaginal wall during the stapling step of the procedure. The use of a vaginal retractor, lifting the vaginal wall in some cases, perpendicular insertion of the device, are important steps to avoid the complication of a recto-vaginal fistula.
FAQs About Rectal Prolapse
Conservative measures may relieve symptoms but surgery is required for definitive treatment.
When performed by an experienced colorectal surgeon, rectal prolapse surgery is safe with good long-term outcomes.
Chronic constipation, pelvic floor weakness, childbirth, and aging are common contributing factors.
Minimally invasive surgery allows faster recovery with most patients returning to normal activities within 2-4 weeks.
Most patients experience significant improvement in bleeding, discharge, and incontinence after surgery.
Rectal Prolapse Surgery in Dubai and Abu Dhabi
Most surgeons carry out rectal prolapse treatment in Dubai and Abu Dhabi. Several techniques are available for the treatment of rectal prolapse and the procedure must be carried out by colorectal surgeons who can best tailor the treatment to each patient. A thorough understanding of the pelvic floor is needed and a multidisciplinary approach with the input of urologists and gynecologists is sometimes needed. The best rectal prolapse surgery in Dubai and Abu Dhabi is offered by fellowship-trained colorectal surgeons with a history of long committed practice in the field.
Looking for a Rectal Prolapse Treatment in Dubai & Abu Dhabi?
A proctology service in Dubai and Abu Dhabi, not only for Rectal Prolapse Treatment but also for many other colorectal conditions, is currently consulting at premier clinics in both cities. Dr. Antonio Privitera is offering free consultations for rectal prolapse treatment in Dubai and Abu Dhabi.
Book an Appointment
