
Colorectal Cancer
What is Colorectal Cancer?
Colorectal cancer affects the large bowel that consists of the colon and rectum. It is the third most common cancer and second most common cause of cancer death worldwide. It affects both men and women and half of the patients are below the age of 65. The 5-year survival rate depends on the stage of the disease that is based on the extent of involvement of the bowel wall, the number of lymph nodes involved, and the presence of metastatic cancer deposits in other organs and structures. In stage 1 and stage II, the survival rate is up to 90%; in stage III up to 70%, and in stage IV only 10%.
Symptoms of Colon and rectal Cancer
Common symptoms of colorectal cancer are recent changes in bowel habits, weight loss, rectal bleeding, abdominal pain, rectal pain, anal pain, the urgency to defecate, anemia, and the presence of a mass. However, colorectal cancer may sometimes give no symptoms, especially in the early stages. A family history of colon and rectal cancer is a risk factor, especially when more than one close family member had cancer, and in particular, if the occurrence was before the age of 50.
Diagnosis of Colon and rectal Cancer
Low rectal cancer and anal cancer can be appreciated on finger examination or seen on visual inspection. A rigid proctoscopy allows for assessment and biopsy of rectal cancer in the clinic. Colonic cancers are assessed and biopsied with flexible endoscopic instruments. A full colonoscopy is essential in all cases to rule out synchronous cancers. CT scan and MRI are used to stage the disease.
Colon and rectal Cancer Screening
There are many screening tests available for colorectal cancer and some can be done at home (fecal occult blood test –FOBT- and fecal immunochemical test – FIT). It is calculated that if 80% of people screened at the age of 50, colorectal cancer fatalities could be reduced by 230,000. As regards colorectal cancer in UAE, it comprises 30% of cancers diagnosed, it is the second most common cancer and the second cause of cancer mortality. As the population of the UAE is young, many cancers are diagnosed at an early age. Colon cancer and rectal cancers in Dubai and Abu Dhabi are on the increase. The Colorectal cancer screening program in Dubai and Abu Dhabi is active and has already been shown to be successful in the early diagnosis of colon and rectal cancer.
There are two ways that screening can reduce colorectal cancer
incidence and mortality. One is to identify the disease at an early
stage when it can be treated with a higher possibility of achieving a
cure. The other is to remove benign polyps by endoscopy before they can
transform into cancer and, therefore, preventing the disease altogether.
Endoscopy in Dubai and Abu Dhabi is performed in many centers with the
gastroenterologists carrying out most of the procedures. However,
colonoscopy is part of the routine practice of a colorectal surgeon in
Dubai and Abu Dhabi. It is difficult to say who is the best surgeon in Dubai and Abu Dhabi to treat colorectal cancer. However, the best colorectal surgeon in Dubai and Abu Dhabi to be
trusted should have at least 10 years of experience of dedicated
colorectal cancer practice in major international institutions, have one
or more fellowships in colorectal surgery, and be part of international
colorectal societies.

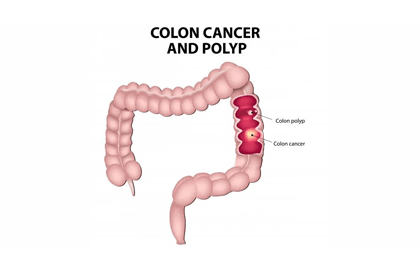
Risks of Colorectal Cancer
Most colon and rectal cancers originate from benign polyps that eventually turn into cancer. This is the reason why everybody should get screened after the age of 50 or at an earlier age if strong family history is present. It takes about 8 years for a benign polyp to become cancer, but this period can be much shorter if particular genetic abnormalities are present.
Some hereditary conditions are linked to a high risk of developing colon and rectal cancer. Familial Adenomatous Polyposis (FAP) is characterized by the presence of multiple polyps that almost invariably will lead to colorectal cancer at a young age. Attenuated forms of this disease have a lower risk of cancer. The other hereditary condition (Hereditary Non-Polyposis Colorectal Cancer –HNPCC) is characterized by genetic mutations that highly increase the risk of colorectal cancer without the presence of multiple polyps. The same genetic mutations can lead to the development of other types of cancer e.g. endometrial, ovarian, gastric, brain, etc.
Chronic inflammation in the colon and rectum may also lead to an increased probability of colon and rectal cancer. Ulcerative colitis and Crohn’s disease are the two inflammatory bowel diseases that are most commonly associated with colorectal cancer. One in five cancer patients is between 20-54 years of age. People born after 1990 are at a much higher risk of developing colon and rectal cancer than those born in the 1950s. It seems that worldwide colon and rectal cancer in the young is becoming more common.
01. Local Excision of Early Cancer
02. Laparoscopic Surgery
03. Robotic Surgery
Colorectal Cancer Treatment
The mainstay of Colorectal cancer is surgery with chemotherapy and radiotherapy used in more advanced cases in the perioperative period. In the case of colon cancer, radiotherapy is not usually an option unless used to radiated a postoperative surgical field at high risk for recurrence. Chemotherapy in colon cancer can be given before surgery to downstage an advanced disease or more commonly postoperatively in early high-risk cancers (e.g. poorly differentiated or with neural and lymphovascular invasion) or in case of lymph node and distant metastases. The survival rate gain with postoperative chemotherapy is around 7%.
In the case of rectal cancer, radiotherapy has been shown to reduce the local recurrence rate, and giving it preoperatively reduces its toxicity. Preoperative combined chemotherapy and radiotherapy is a common regimen used in rectal cancer. Surgery in this case is delayed up to 12 weeks to allow for a complete downstaging of the disease.
If cancer involves only the superficial layers of the bowel wall without the involvement of the muscle, a local excision may be possible in some cases. More commonly surgical treatment involves resection of a segment of the bowel (colectomy or anterior resection) with the surrounding fat-containing potentially involved lymph nodes. This is accomplished by dividing the vessels at their very origin and, in the case of rectal cancer, removing without breaches the surrounding lymph node containing envelope –mesorectum. In the case of the tumor involving other organs and structures (uterus, bladder, small bowel, etc.), it is important to remove the whole tumor in one piece by performing an en-bloc resection. This avoids shedding tumor cells in the surgical field and thus reducing the risk of recurrence. A defunctioning ileostomy or colostomy may be needed after performing a colorectalanastomosis especially if this is close to the anal sphincter complex. In fact, the lower the anastomosis, the higher is the risk of anastomotic leakage that is the most serious complication of colorectal surgery as it is associated with high morbidity and mortality.
FAQs About Colorectal Cancer
Average-risk individuals should begin screening at age 45. Those with family history should start earlier.
Regular colonoscopy screening can prevent cancer by detecting and removing precancerous polyps before they become malignant.
Early colorectal cancer often has no symptoms. Advanced symptoms include rectal bleeding, changes in bowel habits, abdominal pain, and unexplained weight loss.
Treatment depends on stage and may include surgery, chemotherapy, or radiation therapy.
When detected early, colorectal cancer has a 90% survival rate. Early screening is essential.
Looking for a Colorectal Surgeon in Dubai & Abu Dhabi?
A proctology service in Dubai and Abu Dhabi, not only for Colorectal Surgery but also for many other diseases, is currently consulting at premier clinics in both cities. Dr. Antonio Privitera is offering free consultations for colon and rectal cancer patients in Dubai and Abu Dhabi.
Book an Appointment
