
Hernia Surgery
Hernia meaning
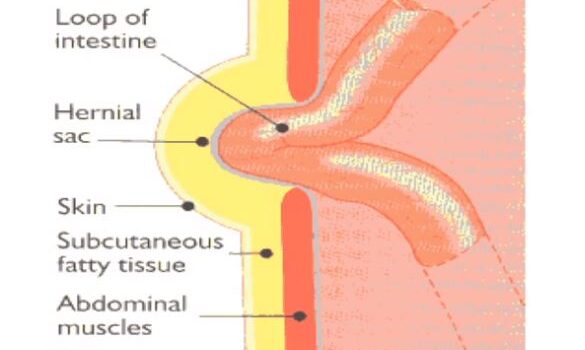
An abdominal wall hernia can be defined as a protrusion of all or part of an intra-abdominal organ or structure through a defect in the Musculo-aponeurotic structures. Hernias can be acquired or congenital depending on whether they develop over the years or they are present at birth. Dr. Antonio is one of the most qualified consultants to perform hernia surgery in Dubai and Abu Dhabi.
Congenital Hernia
Congenital hernias are most commonly inguinal or umbilical and are the result of the failure of closure of the processus vaginalis and the site of passage in the abdominal wall of the umbilical cord respectively.
Congenital inguinal hernias are present in up to 4% of full-term babies and up to 30% of those born prematurely. Males are six times more affected than females. Hernias are usually noted by either the parents while the child is straining/crying or during examination by the pediatrician. Pain and discomfort are usually expressed by infants with cry or irritability. Differential diagnosis must be made with an undescended testis, hydrocele, and lymphadenopathy. Inguinal hernias in infants should be repaired as soon as it is convenient as there is a risk of incarceration and strangulation especially in the first year of life. The hernia operation for congenital inguinal hernias consists of closing the patent peritoneal duct.
Congenital umbilical hernias are present in up to 10% of cases at birth. Incarceration is very uncommon, but they represent a great cause of concern for parents and caregivers as they become very obvious especially when the baby cries. Most of these hernias will resolve spontaneously within the first six years of life. Reassurance must be given to the family and hernia surgery is indicated if the hernia defect eventually fails to close. Plugs or tapes used to keep the hernia reduced with the assumption to speed up closure be not effective and can damage the skin.
hernia Causes
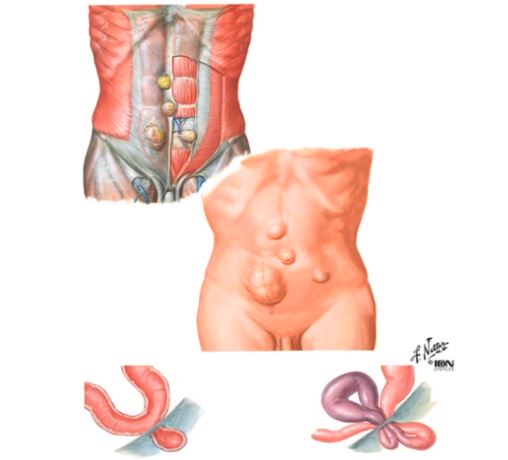
Predisposing factors to abdominal wall hernias are those that produce an increase in intra-abdominal pressure such as straining, heavy lifting, obesity, ascites, chronic cough, and multiple pregnancies. Also, there may be a weakness of the abdominal wall caused by aging, chronic illness, and defects in the metabolism of collagen and extracellular matrix.
Inguinal Hernia
Groin hernias (inguinal and femoral) are the most common as there are natural weak areas in this region caused by the passage of the femoral vessels, the spermatic cord in males, and the round ligament in females. Indirect inguinal hernias pass through the deep inguinal ring and lie lateral to the inferior epigastric vessels. The hernia sac is adherent to the cord structure especially if the acquired hernia develops with time through a partially closed processus vaginalis. Direct hernias are so-called “weakness hernias” as the develop medially to the epigastric vessels due to a weakness of the transversalis fascia. Direct hernias are usually found not adherent to the spermatic cord and they rarely complicate. Groin anatomy is one of the most difficult to learn and master.
Femoral Hernia
Femoral hernias are more common in females and develop through the femoral canal, a space that is bounded laterally by the femoral vein, medially by the lacunar ligament, superiorly by the inguinal ligament, and posteriorly by Cooper’s ligament. They have a higher incidence of incarceration and strangulation.
Epigastric Hernia
Epigastric hernias are upper abdominal hernias that have usually a small defect and develop along the midline raphe. Most of the time the content of the hernia is pre-peritoneal fat. More rarely, omentum or part of upper abdominal organs can be found in it.
Para-Umbilical Hernia
Para-umbilical hernias are acquired hernias that develop on the side of the umbilicus through an area of weakness called Richet’s canal.
Other less commonly encountered abdominal wall hernias include:
- Spigelian Hernia
- Lumbar Hernia
- Obturator Hernia
Hernia Symptoms-Hernia Diagnosis
Hernias may cause pain that is exacerbated by increases of the abdominal pressure (cough, heavy lifting, straining on passing motion). The diagnosis of a hernia is mainly based on clinical examination. Although it may be uncomfortable, introflecting the scrotal skin into the inguinal canal with the finger is the best way to appreciate an inguinal hernia as the full extent of the posterior wall of the inguinal canal can be assessed. Radiological imaging, e.g. ultrasound scan, can be helpful in doubtful cases. A CT scan may be used in obese patients, in cases of emergency or to plan surgical treatment in very large hernias especially those following surgical procedures (incisional).
Acquired hernias can never resolve spontaneously and surgery is the only treatment to address a patient’s symptoms and to avoid the possibility of complications requiring surgical intervention. However, some hernias are more prone to complications than others. Femoral hernias have a high complication rate as the defect is small and mainly bounded by aponeurotic rigid structures. Direct inguinal hernias are incarcerated or strangulate very rarely.with
Complications with hernias
Complications of hernias include irreducibility, obstruction, and strangulation. When a hernia becomes irreducible, the hernia sac with its content cannot be pushed back into the abdominal cavity. This is usually caused by adhesions of the sac with the surrounding structures or between the sac and its content. Hernias with a small defect are more likely to become irreducible. Intestinal hernia content may be complicated by bowel obstruction presenting with abdominal pain, distension, obstipation, nausea, and vomiting. If the blood supply to the content becomes impaired, strangulation ensues and this may lead to gangrene and perforation. This is a life-threatening condition and requires emergency surgery.
Hernia Treatment
Conservative management of hernias is to be considered only in few selected cases, e.g. poorly symptomatic hernias in patients at high risk for surgery. Otherwise, hernia surgery should be advised in most cases.
An Overview of Hernia Surgery
Minimally Invasive Techniques In Hernia Surgery
Hernia surgery can be performed open or using minimally invasive techniques including laparoscopic and robotic techniques. Although hernia surgery is classically one of the most common general surgery operations and performed by any surgeons, results are seen to be much better in the hands of a surgeon having a particular interest in the field. Therefore, in the last 20 years, many hernia surgery centers have been created with some surgeons completely devoting their practice to hernia treatment.
Prosthetic Materials (Mesh) in Hernia Surgery
In general, the use of prosthetic materials (mesh) in hernia surgery is the standard treatment as it is associated with a low recurrence rate. Meshes can be placed over the musculoaponeurotic abdominal wall structures (on-lay repair), in-between them (inlay repair), or below them (sub-lay repair). Before the introduction of meshes, the recurrence rate of hernias was high. This is because when a suture only repair is performed, there are two risk factors for recurrence that must be considered. One is the tissue tension created by closing the defect and the other the weakness of the aponeurotic structures that in itself is a predisposing factor for hernia formation. As regards inguinal hernias, Bassini’s repair was the first hernia surgery repair described in the literature and was revolutionary. The concept of closing the defect in the posterior wall of the inguinal canal by approximating the conjoint tendon or the inferior margin of the internal oblique and transversus abdominis to the inguinal ligament represented a milestone. The main drawback of this kind of repair is the tension that is created that is the prime etiological factor for hernia recurrence. Other surgeons, e.g. Shouldice, developed techniques of suture repair that helped to distribute the tension in several layers and thus achieving low recurrence rates.
Lichtenstein Hernia Mesh Technique in hernia Surgery
The Lichtenstein hernia mesh technique with the apposition of a mesh to cover the defect (without closing it) was again a milestone in hernia surgery and gave way to the widespread use of prosthetic materials and the introduction of a wide variety of techniques by other surgeons. The recurrence rate of Lichtenstein repair for inguinal hernia is less than 1%.
Inguinal Hernia Surgery
Regardless of the technique used to repair inguinal hernias, it is of paramount importance to identify and protect the nerves that are at risk of being injured during the surgery thus avoiding postoperative complications such as chronic postoperative pain and/or reduced local sensation. There are three nerves encountered during inguinal hernia surgery: the ilioinguinal nerve that runs on the anterior surface of the spermatic cord, the genital branch of the genitor-femoral nerve that runs in the posterior part of the cord, and the iliohypogastric nerve that can be found on the anterior surface of the internal oblique muscle. Encompassing the nerve with a stitch when it is still in continuity is a major cause of chronic postoperative pain (neuralgia) that is of difficult solution.
Laparoscopic Hernia Treatment
The advent of laparoscopy revolutionized hernia treatment. Laparoscopy has the main advantage of reducing pain after surgery, earlier return to normal life, and better cosmesis. During the laparoscopic repair of an inguinal hernia using a transabdominal approach (TAPP), a preperitoneal pocket is created and the hernia sac is dissected out and reduced/ excised. The peritoneum is then closed with absorbable tacks or sutures. This approach allows us to address bilateral hernias using the same incisions and to repair both inguinal and femoral hernias.
FAQs About Hernia Surgery
No. Hernias do not heal on their own.
Surgery is the only definitive treatment to
prevent serious complications like strangulation.
Modern laparoscopic hernia repair causes
minimal pain. Discomfort is managed effectively
with oral pain medications and typically resolves
within days.
Desk job patients can return within 1-2 weeks.
Those doing manual labor may need 4-6 weeks.
Laparoscopic repair allows faster recovery than
open surgery.
Modern mesh repair has over 95% success rate
with less than 5% recurrence when performed by
an experienced surgeon like Dr. Antonio.
Laparoscopic repair offers smaller incisions,
less pain, and faster recovery. Dr. Antonio recommends
the most appropriate approach based on each
patient’s individual condition.
Hernia Surgery in Dubai & Abu Dhabi
Hernia operations are very commonly performed in Dubai and Abu Dhabi by most surgeons. However, patients must be aware that the best results are achieved by surgeons with a specific interest in this type of surgery, and the best hernia surgery specialist in Dubai and Abu Dhabi to carry out the procedure should be sought.
Hernia surgery in Dubai and Abu Dhabi is still in the hands of general specialists and that is why results can sometimes be erratic and uncontrolled. Dr. Antonio is one of the most qualified consultants to perform hernia surgery in Dubai and Abu Dhabi. He holds an MD and Ph.D. in hernias and he is the author of numerous peer-reviewed research in the field. He pioneered a novel plug-technique for the treatment of umbilical and a double-layer mesh technique for lumbar hernias. Together with Prof. Angelo Donati in Italy, he pioneered the “Calibrated inguinal hernia repair” that was presented in several national and international conferences. He also worked with Prof. Andrew Kingsnorth, former President of the European Hernia Society.
Looking for a Hernia Doctor in Dubai & Abu Dhabi?
A proctology service not only for Hernia Surgery in Dubai and Abu Dhabi but also for many other diseases is currently available at leading hospitals in the region. Dr. Antonio Privitera is offering a free consultation for hernia treatment in Dubai and Abu Dhabi.
Book an Appointment
