
Most patients with an anal fissure can be treated with topical creams. Before exploring specific medications, our anal fissure treatment in Dubai explains how treatment is matched to the type and stage of fissure.
If the right cream is chosen, applied correctly, and used for long enough. The problem is that patients often either use the wrong product (hemorrhoid cream, which does nothing for fissures), use the right cream incorrectly, or stop too soon.
This guide covers every pharmacological option for anal fissure treatment, with evidence, dosing, and practical guidance.
How Topical Creams Work
Anal fissure pain and failure to heal are caused by internal sphincter spasm, which reduces blood supply to the posterior midline. Topical creams work by relaxing the internal sphincter reducing pressure, restoring blood supply, and creating conditions in which the tear can heal. They do NOT simply numb the area.
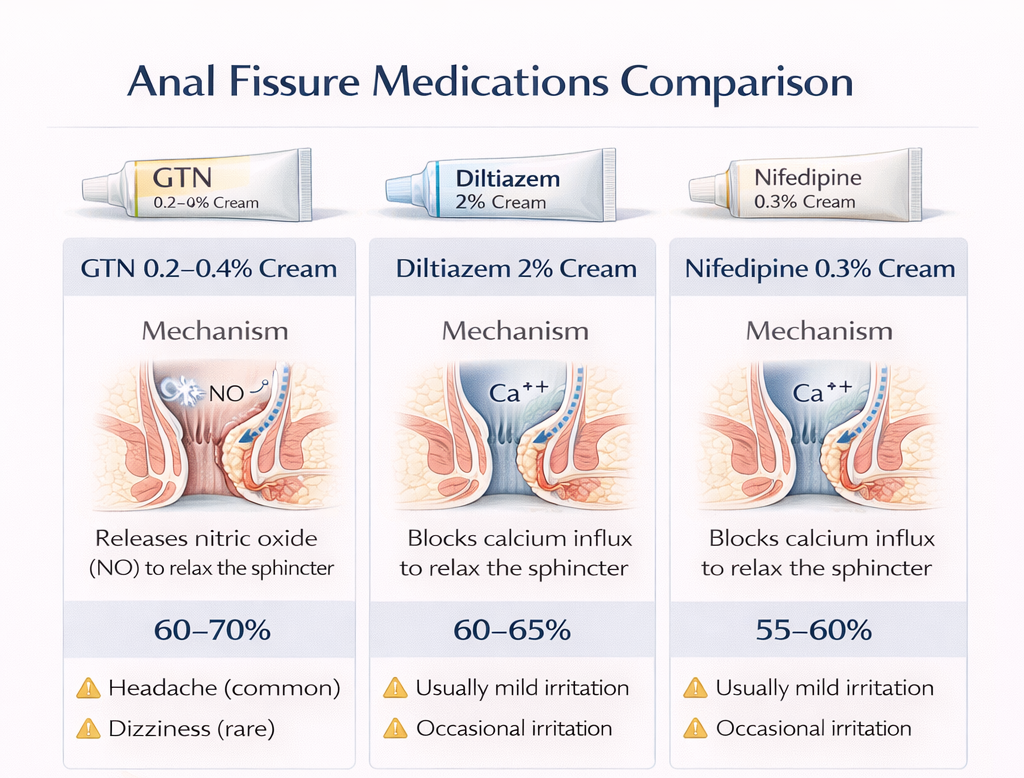
First-Line Treatment: Glyceryl Trinitrate (GTN) Cream
How It Works
GTN is a nitric oxide donor. Nitric oxide relaxes smooth muscle including the internal anal sphincter. Applied topically to the anal canal, GTN reduces resting anal pressure by 20-30%.
Dosing
- Concentration: 0.2% or 0.4% (0.4% is more effective but causes more headaches)
- Frequency: Twice to three times daily, including after bowel movements
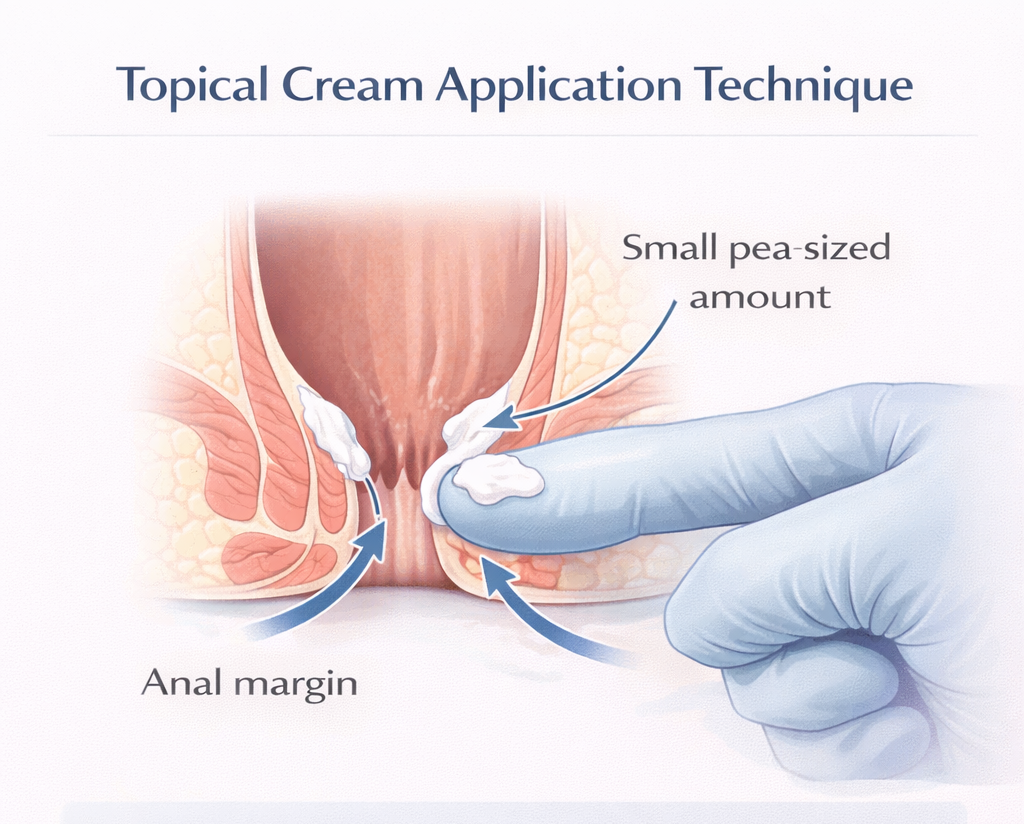
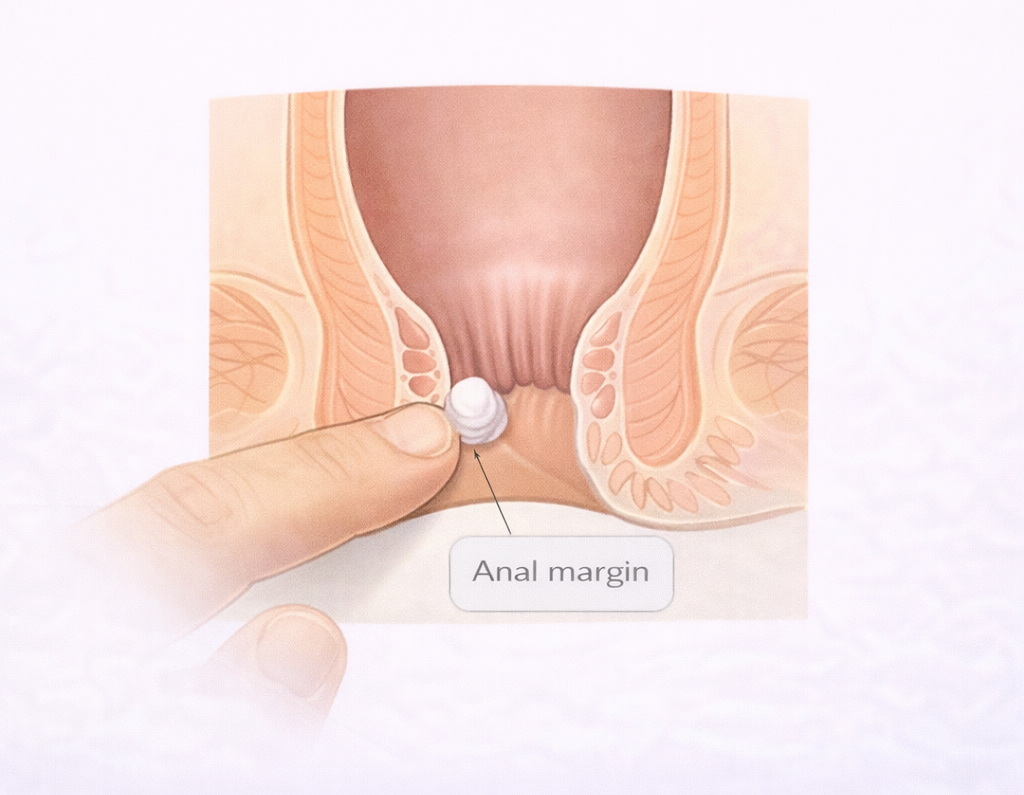
- Amount: A small pea-sized amount applied just inside and around the anal margin
- Duration: 6-8 weeks continuous use
Efficacy
Healing rate: 60-70% for acute fissures. Lower for chronic fissures (around 40-50%) still worth attempting as first line.
Side Effects
- Headache: The most common side effect reported by up to 40% of patients at 0.4%. Usually mild and dose-related. Using a smaller amount reduces it.
- Dizziness: Less common; avoid applying and then standing up suddenly.
Second-Line or Alternative: Diltiazem 2% Cream
How It Works
Diltiazem is a calcium channel blocker that reduces calcium influx into smooth muscle cells, causing sphincter relaxation.
Dosing
- Concentration: 2%
- Frequency: Twice daily
- Duration: 6-8 weeks
Efficacy
Healing rate: Similar to GTN approximately 65%. Some studies suggest slightly lower than GTN, others show equivalent efficacy.
Advantage Over GTN
Significantly fewer headaches. Preferred for patients who cannot tolerate GTN. Available as topical cream or oral diltiazem (oral is less effective for fissure; topical is preferred).
Alternative: Nifedipine 0.3% Cream
Another calcium channel blocker. Smaller evidence base than diltiazem. Used when diltiazem is unavailable or ineffective.
Topical Anesthetics: For Symptom Relief, Not Healing
Lidocaine (lignocaine) 5% gel or ointment applied before bowel movements reduces pain. It does NOT treat the fissure it only makes bowel movements more tolerable while other treatments work.
- Useful as an adjunct to GTN or diltiazem
- Do not rely on it as sole treatment it will not heal the fissure
Stool Softeners and Fiber Supplements
- Lactulose: Osmotic laxative draws water into the bowel
- Macrogol (PEG): Effective, well-tolerated stool softener
- Docusate sodium: Surfactant laxative softens stool by allowing water penetration
- Psyllium husk (Metamucil / Fybogel): Bulk-forming fiber supplement best long-term option
When Creams Are Not Enough
If you have used GTN or diltiazem correctly for 6–8 weeks and the fissure has not healed, the next step is Botox injection — not more cream. If creams fail, Botox injection for anal fissure in Dubai is the next step. Surgical treatment involves lateral internal sphincterotomy in Dubai.
Need expert treatment for hemorrhoids, anal fissure, or anal fistula? Book a consultation with Dr. Antonio Privitera in Dubai or Abu Dhabi.
📱 WhatsApp: +971 55 318 8469
📞 Phone: +971 55 318 8469
AUTHOR AUTHORITY BLOCK
Fellowship-trained at Mayo Clinic (USA) and the Royal College of Surgeons (UK). Member of the Royal College of Surgeons of Edinburgh. Certified in General Surgery by the Italian Medical Council.
About the Author
