
Anal fissures are a common cause of severe anal pain, especially during and after bowel movements. For a complete overview of diagnosis and treatment, this page explains the causes, symptoms, and the most effective treatment options available.
I’m Professor Dr. Antonio Privitera, a consultant colorectal surgeon with fellowship training at the Mayo Clinic and in London, and European Board Certification in Colorectal Surgery. I specialize in the diagnosis and treatment of anal fissures, hemorrhoids, anal fistulas, and other anorectal conditions.
Here is what you need to know:
- Most anal fissures are not dangerous, but they do not heal on their own without treatment.
- The pain is caused by spasm of the internal sphincter muscle, not just the tear itself
- Non-surgical treatment works for most patients: creams, Botox, and dietary changes.
- Surgery (LIS) is reserved for chronic fissures that do not respond to conservative treatment
- Accurate diagnosis matters-not all anal pain or rectal bleeding is a fissure
What Is an Anal Fissure?
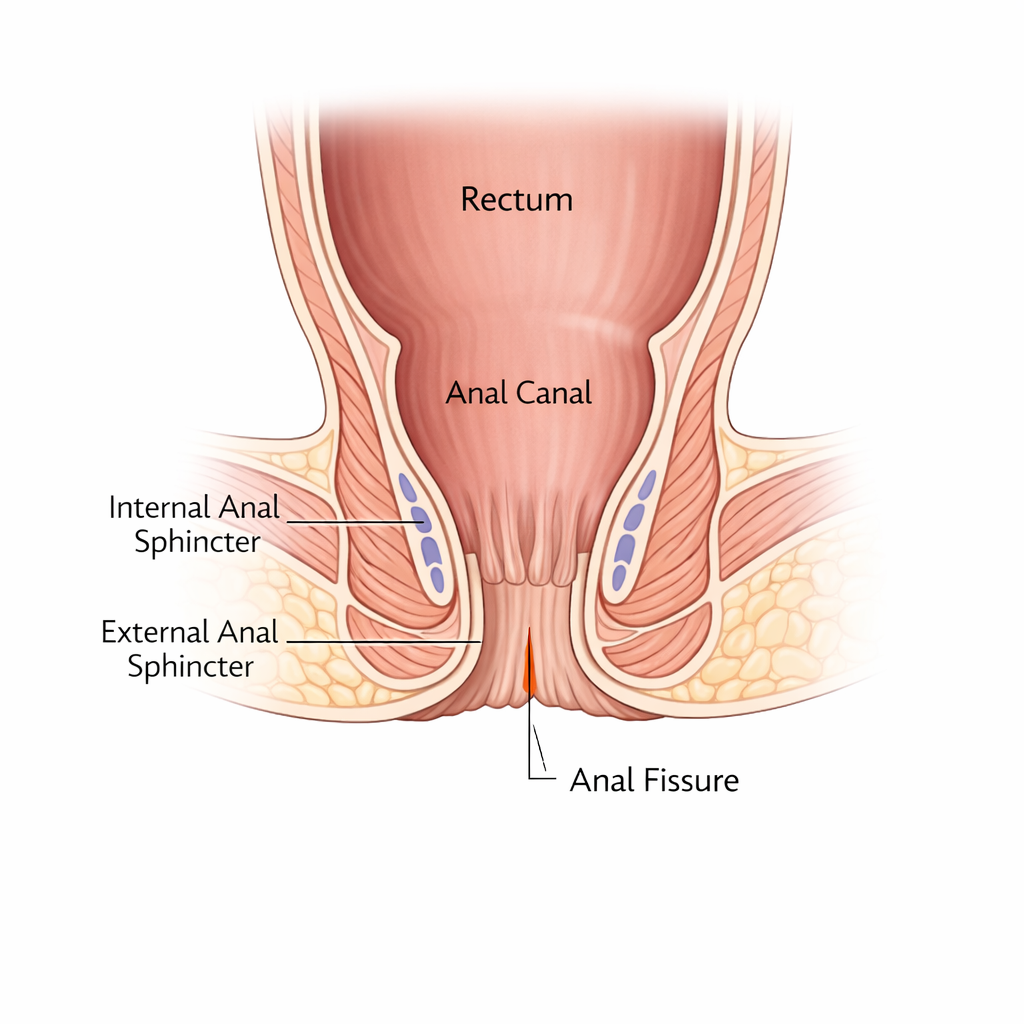
An anal fissure is a small tear in the lining of the anal canal, the short tube that connects the rectum to the outside. The tear usually occurs at the posterior midline (the 6 o’clock position when you are lying on your back), though it can also occur at the anterior midline, particularly in women.
The tear causes the internal anal sphincter (the involuntary muscle that keeps the anus closed) to go into spasm. This spasm reduces blood supply to the area, which prevents healing and causes the severe, prolonged pain that patients describe.
Acute vs Chronic Anal Fissure
- Acute fissure: Lasts less than 6 weeks. Edges are clean and fresh. High chance of healing with conservative treatment.
- Chronic fissure: Lasts more than 6 weeks. Develops a sentinel pile (skin tag) at the outer edge and a hypertrophied anal papilla at the inner edge. Requires more aggressive treatment.
Chronic fissures behave differently. See why fissures don’t heal.
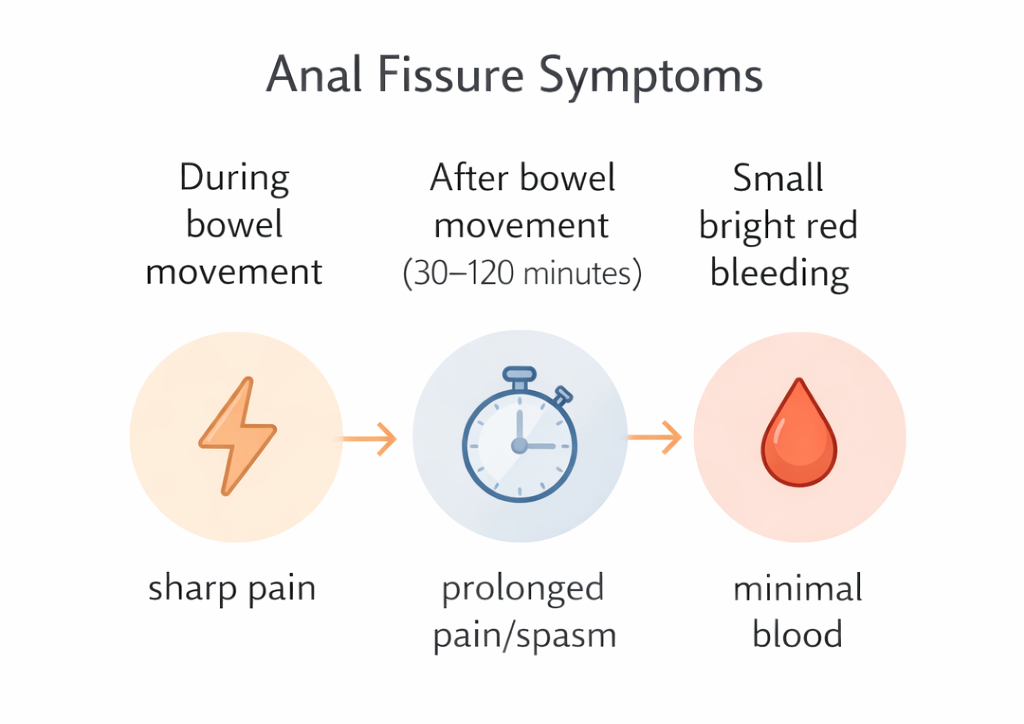
Symptoms: What You Will Notice
- Sharp, tearing pain during bowel movements often described as ‘passing glass’ or ‘a knife cutting’
- Pain that continues for 30 minutes to 2 hours after the bowel movement (sphincter spasm)
- Bright red blood on toilet paper or on the surface of stool usually small amounts
- Itching or burning around the anus
- Fear of going to the toilet – avoidance behavior that worsens constipation and makes healing harder
If symptoms are severe or persistent, specialist evaluation is recommended.
What Causes Anal Fissures?
- Passing a hard, large stool – the most common cause
- Chronic constipation and straining
- Diarrhea – repeated loose stools irritate the anal lining
- Childbirth – particularly with perineal trauma
- Low fiber diet and dehydration – very common in Dubai’s population
- Tight internal anal sphincter – some people have a higher resting anal pressure, which reduces blood supply to the posterior midline
Treatment Options in Dubai
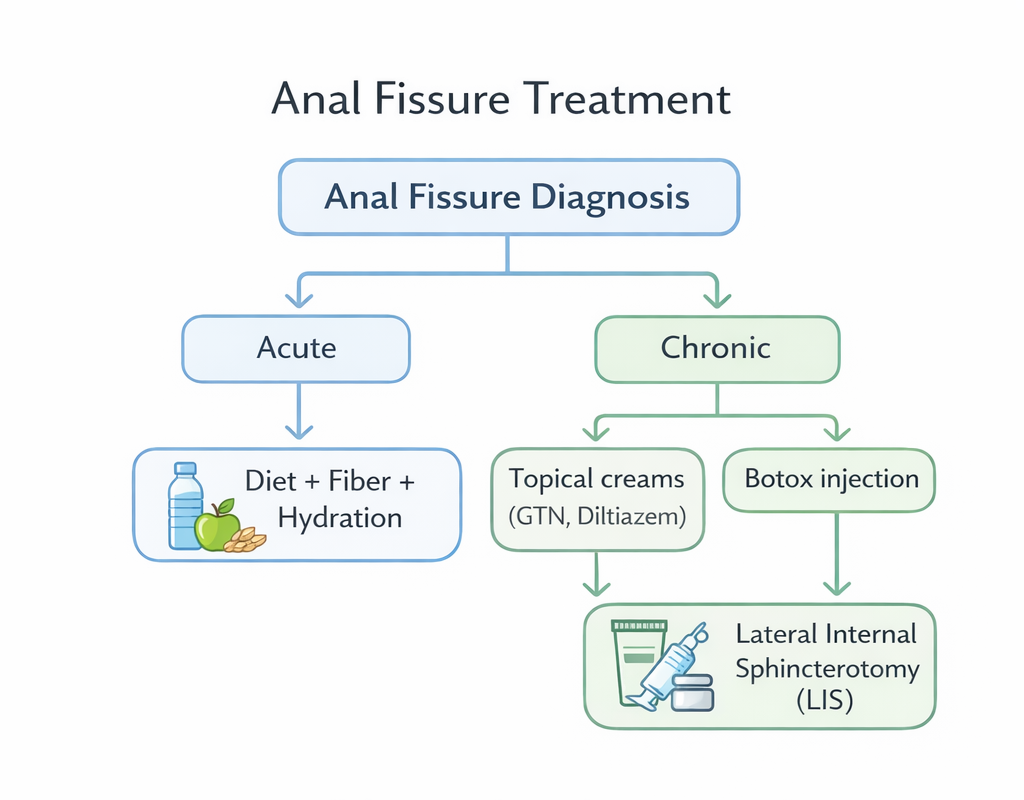
Conservative Treatment (First Line – All Acute Fissures)
- High-fiber diet: 25-35 grams of fiber daily – fruits, vegetables, legumes, whole grains
- Hydration: 2.5-3 liters of water daily – Dubai’s heat increases dehydration risk
- Stool softeners: Lactulose, macrogol, or docusate if needed
- Sitz baths: Warm (not hot) water for 10-15 minutes after bowel movements relaxes the sphincter
- Topical anesthetics: Lidocaine cream before bowel movements to reduce pain
Topical Creams (First and Second Line)
The goal of topical creams is to relax the internal sphincter, improve blood supply, and allow healing:
- Glyceryl trinitrate (GTN) 0.2-0.4%: First-line pharmacological treatment. Relaxes the sphincter. Side effect: headache (common).
- Diltiazem 2%: Calcium channel blocker. Similar efficacy to GTN, fewer headaches. Often preferred for patients who cannot tolerate GTN.
- Nifedipine 0.3% cream: Alternative calcium channel blocker.
Botox Injection
A Botox injection for anal fissure in Dubai into the internal sphincter temporarily paralyses it, reducing spasm and allowing blood supply – and healing – to recover. Done in clinic or under brief sedation. Effective for chronic fissures that have not healed with creams.
Lateral Internal Sphincterotomy (LIS) – Surgical Treatment
Lateral Internal Sphincterotomy Dubai involves a small surgical cut in the internal sphincter to permanently reduce sphincter pressure. Healing rate exceeds 95%. Reserved for chronic fissures that do not respond to medical treatment. Risk of minor incontinence is low but must be discussed.
When to See a Specialist
If you have had anal pain and bleeding for more than 4 weeks without improvement with dietary changes and over-the-counter creams, you need specialist evaluation. Early treatment prevents a simple acute fissure from becoming a chronic one.
Frequently Asked Questions
Can an anal fissure heal on its own?
Acute fissures can heal with dietary changes and topical treatment. Chronic fissures (lasting more than 6 weeks) rarely heal without medical or surgical intervention.
Is surgery always required?
No. Most fissures respond to creams and dietary changes. Surgery is reserved for chronic fissures that fail conservative treatment.
How long does treatment take?
Acute fissures may heal in 4-8 weeks with treatment. Chronic fissures take longer and may require Botox or LIS.
References
- National Institute for Health and Care Excellence (NICE). Anal fissure. 2021.
- American Society of Colon and Rectal Surgeons (ASCRS). Practice parameters for the management of anal fissures. Dis Colon Rectum. 2017.
- Nelson RL et al. Non surgical therapy for anal fissure. Cochrane Database Syst Rev. 2012.
Need expert treatment for hemorrhoids, anal fissure, or anal fistula? Book a consultation with Dr. Antonio Privitera in Dubai or Abu Dhabi.
📱 WhatsApp: +971 55 318 8469
📞 Phone: +971 55 318 8469
AUTHOR AUTHORITY BLOCK
Fellowship-trained at Mayo Clinic (USA) and the Royal College of Surgeons (UK). Member of the Royal College of Surgeons of Edinburgh. Certified in General Surgery by the Italian Medical Council.
About the Author
