
Acute and chronic anal fissures differ in duration, appearance, and treatment approach. Understanding the difference helps guide correct management. For full treatment pathways, see anal fissure treatment in Dubai.
Some patients confuse fissure pain with hemorrhoids – see hemorrhoid treatment in Dubai for comparison. This guide explains the clinical differences between acute and chronic anal fissures, how each is diagnosed, and how treatment differs.
Acute Anal Fissure: What It Looks Like
Definition
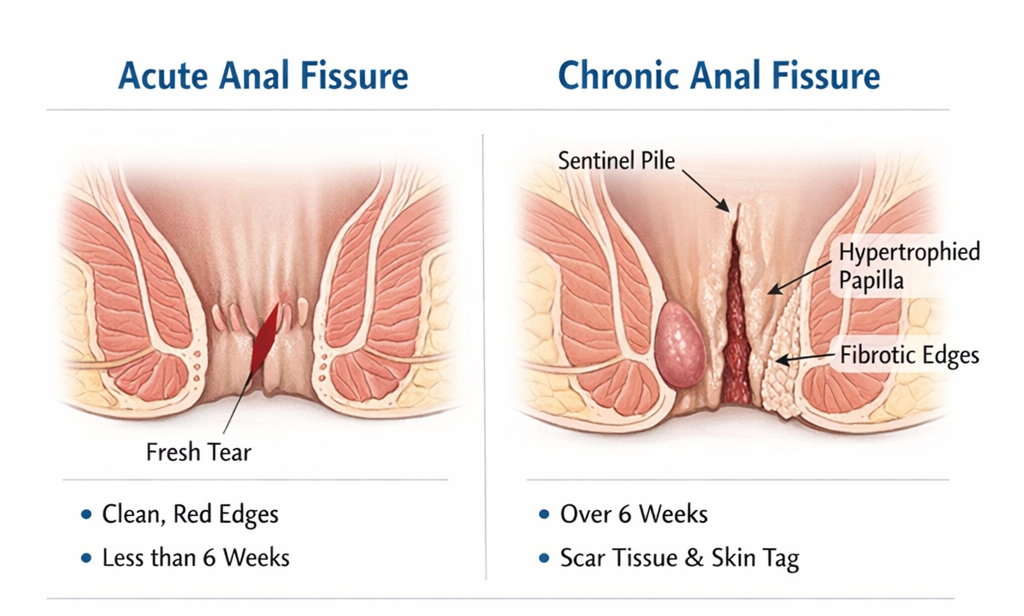
An acute fissure has been present for less than 6 weeks. It is a fresh tear with clean, soft edges like a paper cut in the anal lining.
Clinical Features
- Sharp pain during and shortly after bowel movements (spasm lasts 30-90 minutes)
- Small amount of bright red blood on toilet paper
- Tender, fresh-looking tear on examination – usually at the posterior midline (6 o’clock position)
- No skin tag (sentinel pile) or hypertrophied papilla
Prognosis
With appropriate treatment – high-fiber diet, adequate hydration, topical creams – most acute fissures heal within 4-8 weeks. The key is starting treatment early before the fissure becomes chronic.
Chronic Anal Fissure: What It Looks Like
Definition
A chronic fissure has been present for more than 6 weeks, or has recurred multiple times. Repeated cycles of spasm and failed healing cause structural changes that prevent natural healing.
Clinical Features
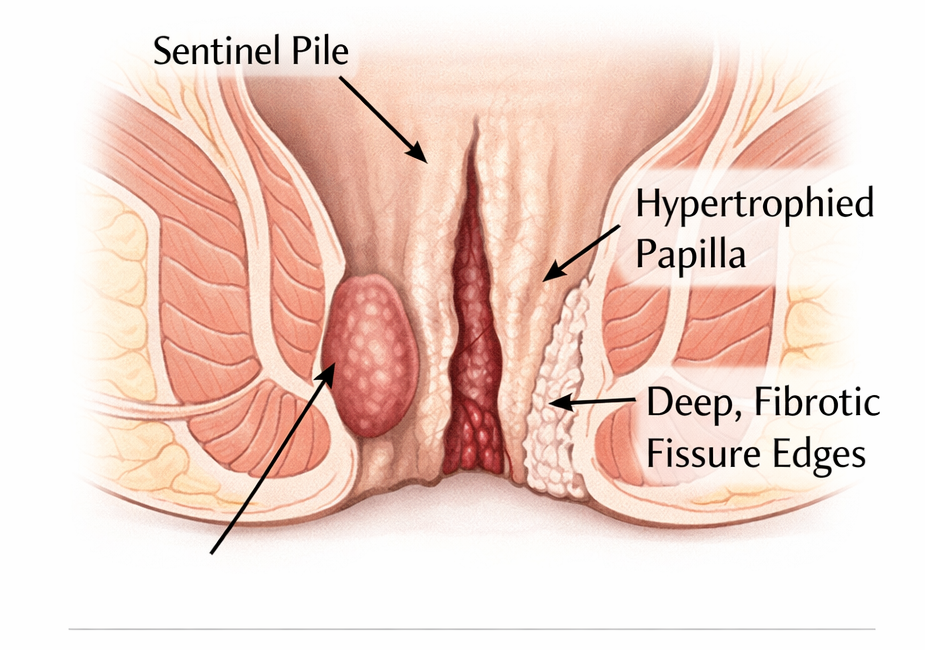
- Visible sentinel pile (skin tag) at the outer edge of the fissure – this is the hallmark of chronicity
- Hypertrophied (enlarged) anal papilla at the inner edge
- Deep, fibrotic edges – the fissure looks pale or white due to exposed internal sphincter muscle
- Symptoms may be severe or surprisingly mild – some patients have large chronic fissures with only moderate pain
Why Chronic Fissures Don’t Heal
Three factors conspire against healing:
- High sphincter pressure: Persistent spasm reduces blood supply to the posterior midline – the area is already poorly vascularized to begin with.
- Fibrosis: The edges of a chronic fissure become scarred and rigid, preventing the epithelium from bridging the gap.
- Infection: Secondary infection with skin flora can maintain inflammation and perpetuate the cycle.
Diagnosis: How the Distinction Is Made
Diagnosis is clinical-based on history and examination. A digital rectal exam and anoscopy allow assessment of:
- Fissure location and appearance
- Presence or absence of a sentinel pile
- Internal sphincter tone (tight = high resting pressure = higher risk of chronicity and poor healing)
- Other conditions – hemorrhoids, fistula, polyp
Treatment Differences
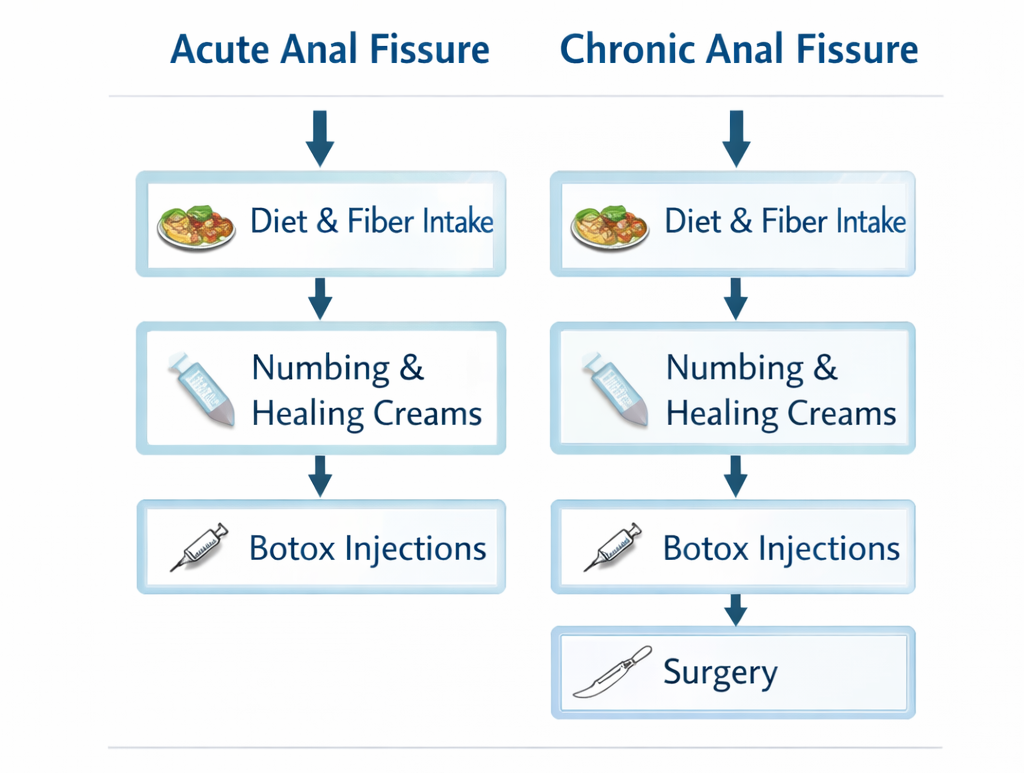
- Acute Fissure:
- High-fiber diet + hydration
- Topical GTN 0.2-0.4% or diltiazem 2% cream for 6-8 weeks
- Warm sitz baths after bowel movements
- Stool softeners if constipation is present
- Healing expected in 4-8 weeks in most patients
- Chronic Fissure:
- Continue dietary measures (they support healing regardless)
- Topical creams: still worth trying for 6-8 weeks if not previously attempted
- Botox injection in Dubai: preferred second-line treatment – effective in 60-70% of chronic fissures
- Lateral internal sphincterotomy (LIS) in Dubai: surgical treatment with >95% healing rate – reserved for fissures that fail Botox or present with very high sphincter pressure
References
- American Society of Colon and Rectal Surgeons (ASCRS). Practice parameters for the management of anal fissures. Dis Colon Rectum. 2017.
- Madoff RD, Fleshman JW. Clinical practice. Anal fissure. N Engl J Med. 2003.
Need expert treatment for hemorrhoids, anal fissure, or anal fistula? Book a consultation with Dr. Antonio Privitera in Dubai or Abu Dhabi.
📱 WhatsApp: +971 55 318 8469
📞 Phone: +971 55 318 8469
AUTHOR AUTHORITY BLOCK
Fellowship-trained at Mayo Clinic (USA) and the Royal College of Surgeons (UK). Member of the Royal College of Surgeons of Edinburgh. Certified in General Surgery by the Italian Medical Council.
About the Author
