
Anal fissures have a specific, well-understood cause: the anal canal is stretched beyond its capacity, the lining tears, and the underlying sphincter goes into spasm. Understanding what drives this process helps you treat and prevent fissures and helps you have an honest conversation with your specialist about which factors apply to your situation.
For a complete overview of fissure diagnosis and all treatment options, see our anal fissure treatment guide in Dubai.
I’m Professor Dr. Antonio Privitera, a consultant colorectal surgeon practicing in Dubai and Abu Dhabi. This article explains every cause of anal fissures, including factors that are particularly common in the UAE.
The Mechanism: Why Fissures Form and Why They Don’t Heal
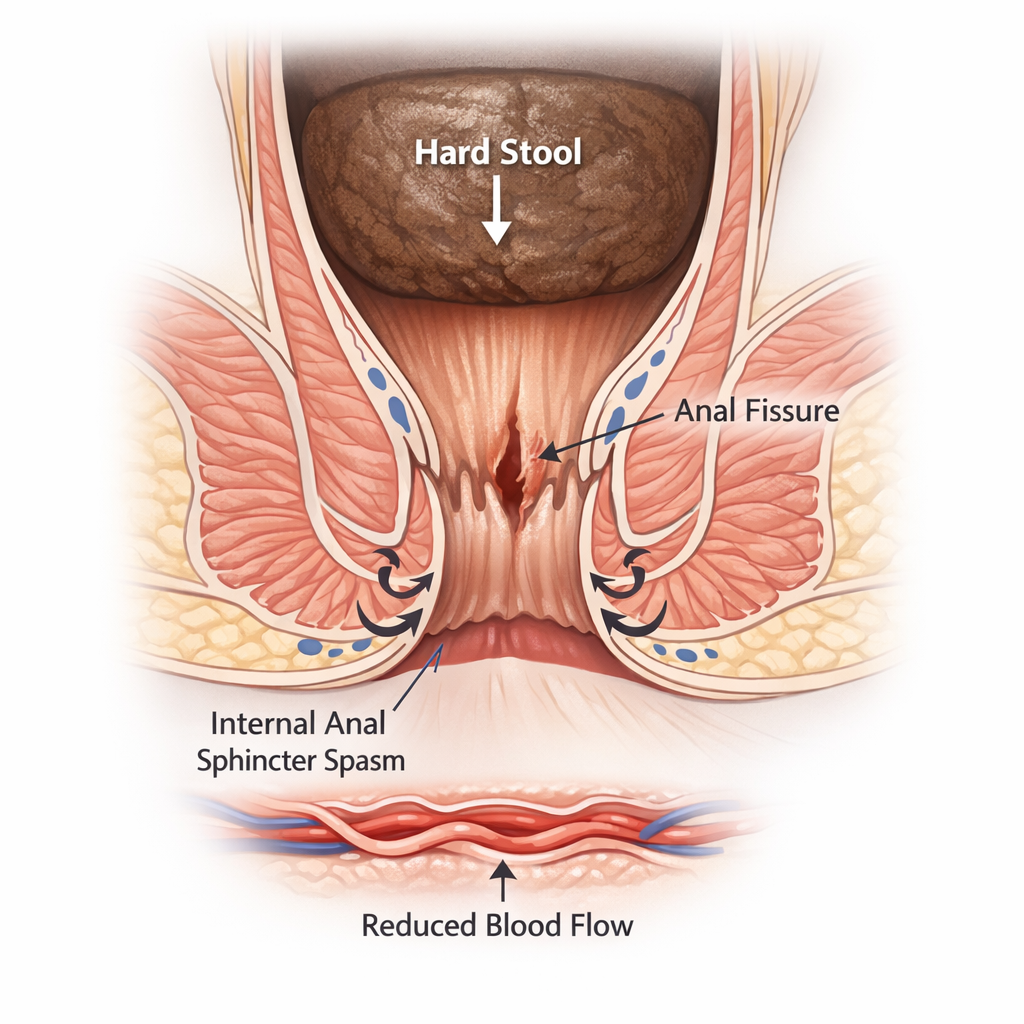
The anal canal lining tears when it is stretched beyond its capacity usually by a hard, large stool. The internal anal sphincter (an involuntary circular muscle) immediately goes into spasm in response to the tear. This spasm:
- Increases pressure inside the anal canal
- Reduces blood supply to the posterior midline, the area where fissures almost always form.
- Prevents the tear from healing
- Causes the prolonged pain (often 30-60 minutes after a bowel movement) that fissure patients describe
This cycle – tear → spasm → reduced blood supply → failed healing – is why an untreated fissure becomes chronic.
Chronic fissures behave differently. See why fissures don’t heal.
Primary Causes (Most Common)
1. Hard or Large Stools
The single most common trigger. When you pass a large, hard, or poorly lubricated stool, the anal canal stretches suddenly and tears. Risk factors:
- Low fiber diet
- Dehydration, particularly relevant in Dubai’s climate.
- Sedentary lifestyle
- Reduced bowel movement frequency
2. Chronic Constipation and Straining
Repeatedly straining to pass stool increases anal canal pressure, injures the lining, and promotes fissure formation. Constipation also means less frequent stools that are harder and larger when they do come.
3. Chronic Diarrhea
Repeated loose, acidic stools irritate and erode the anal lining. Patients with IBS, IBD, or food intolerances are at increased risk.
4. High Internal Sphincter Pressure (Hypertonia)
Some people have a constitutionally tight internal sphincter with high resting pressure. This reduces blood supply to the posterior midline, making it more vulnerable to tearing and less capable of healing.
Treatment options vary. See Botox treatment.
Contributing Factors in the UAE
Low Fiber Diet
Many patients in Dubai eat out frequently or rely on processed foods that are low in fiber. The recommended intake is 25-35 grams daily; most people consume far less.
Dehydration
Dubai’s heat, air conditioning, and a reliance on coffee and tea rather than water all contribute to dehydration which directly hardens stools.
Sedentary Office Work
Long hours sitting in air-conditioned offices reduces bowel motility and predisposes to constipation.
Specific Populations at Higher Risk
Women After Childbirth
Perineal trauma during vaginal delivery particularly with second-degree or third-degree tears can involve the anal canal and produce anterior fissures. Hormonal changes also affect anal sphincter tone.
Patients with Crohn’s Disease
In Crohn’s disease, inflammation occurs throughout the GI tract including the perianal area. Fissures in Crohn’s patients are often atypical — multiple, lateral, deep, and with undermined edges. They require specialist management distinct from ordinary fissures.
Older Adults
Reduced anal sphincter tone and slower bowel transit increase risk.
Secondary Causes (Less Common)
- Anal surgery – prior hemorrhoidectomy or fistula repair can cause scarring that reduces anal canal compliance
- Sexually transmitted infections – herpes, syphilis, chlamydia can all cause anal ulceration resembling fissures
- HIV/AIDS – atypical fissures with poor healing
- Tuberculosis – rare but important in high-prevalence populations
- Anal cancer – any non-healing anal ulcer that does not respond to treatment must be biopsied
Important: If you have an anal fissure that does not respond to standard treatment within 6-8 weeks, specialist evaluation and possible biopsy are required to exclude malignancy or specific infection.
When conservative measures fail, Botox injection for anal fissure in Dubai is the next step.
References
- Mapel DW et al. The epidemiology and treatment of anal fissures in a population-based cohort. BMC Gastroenterol. 2014.
- Lund JN, Scholefield JH. Etiology and treatment of anal fissure. Br J Surg. 1996.
Need expert treatment for hemorrhoids, anal fissure, or anal fistula? Book a consultation with Dr. Antonio Privitera in Dubai or Abu Dhabi.
📱 WhatsApp: +971 55 318 8469
📞 Phone: +971 55 318 8469
AUTHOR AUTHORITY BLOCK
Fellowship-trained at Mayo Clinic (USA) and the Royal College of Surgeons (UK). Member of the Royal College of Surgeons of Edinburgh. Certified in General Surgery by the Italian Medical Council.
About the Author
