
Complex anal fistulas require specialist surgical planning to achieve cure while preserving continence. For full treatment options, see anal fistula treatment in Dubai.
What Makes a Fistula ‘Complex’?
- High transsphincteric – involves upper 2/3 of external sphincter
- Suprasphincteric or extrasphincteric fistulas
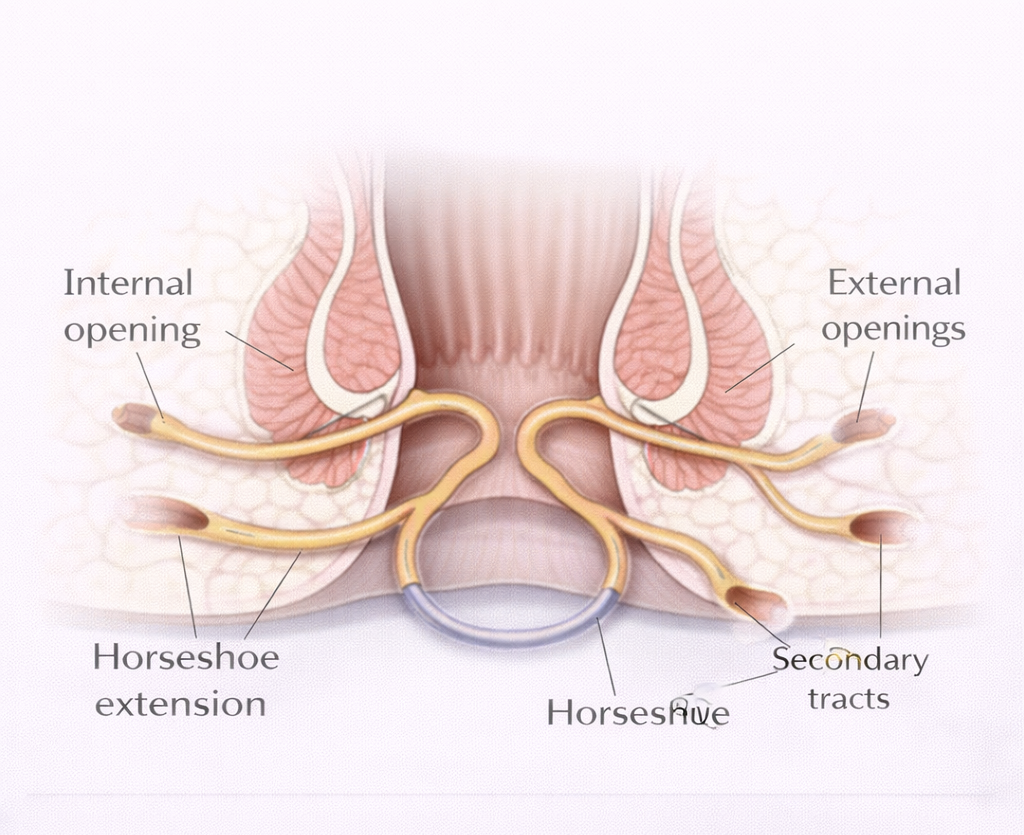
- Multiple external openings or secondary tracts (horseshoe extension)
- Previous failed fistula surgery
- Crohn’s disease
- Female patient with anterior fistula (short anterior perineum)
- Pre-existing sphincter weakness or incontinence
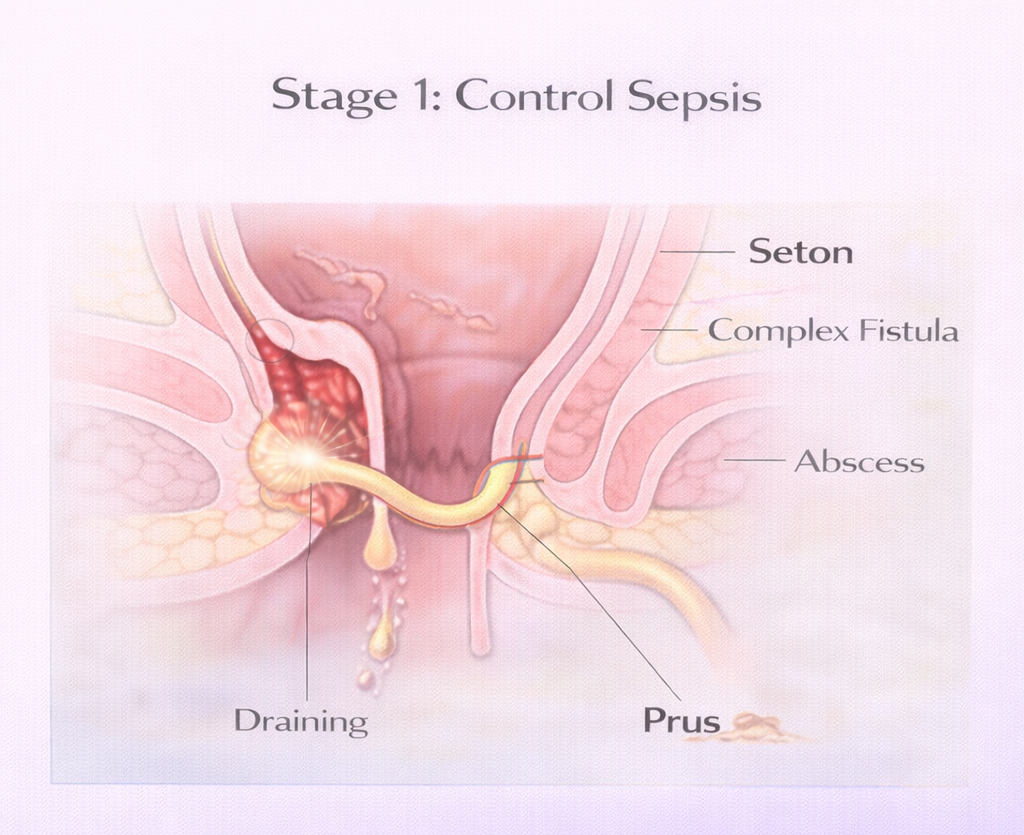
Stage 1: Control Sepsis
Before definitive repair of any complex fistula, active infection must be controlled. This usually means:
- Seton Fistula Dubai – Draining (loose) seton placement:
Keeps the tract open, allows drainage, eliminates acute sepsis
- Any abscess collections must be drained
- MRI reassessment once sepsis controlled to plan definitive repair
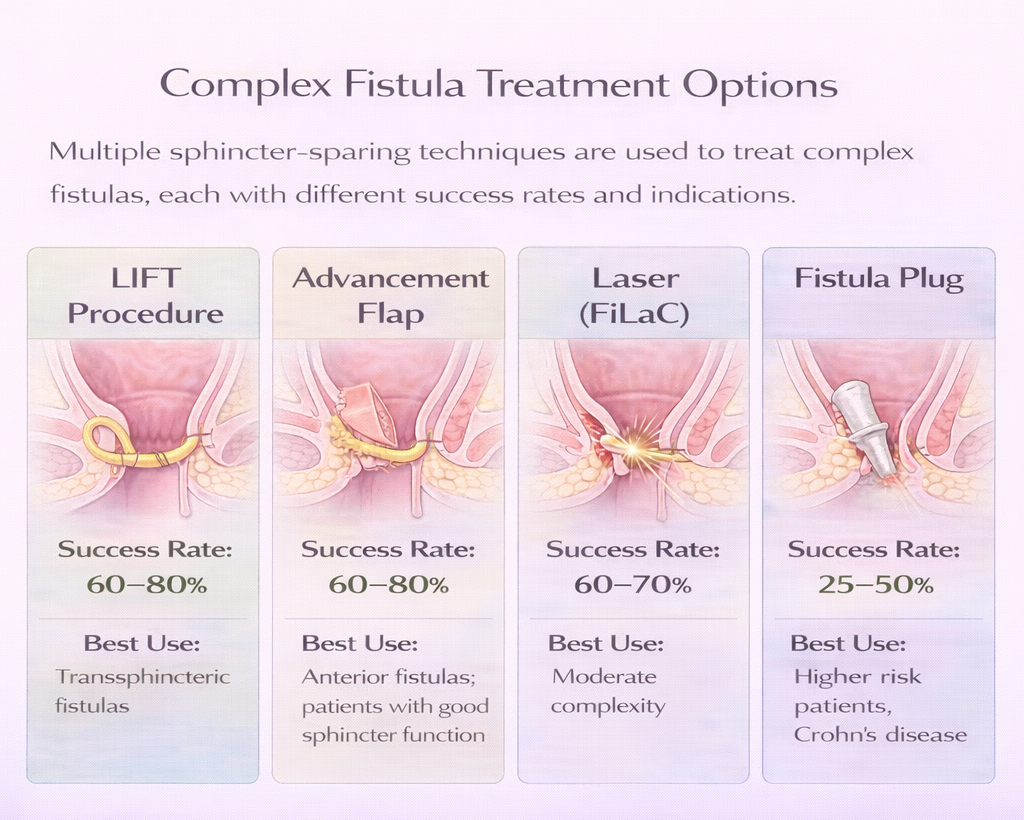
Stage 2: Definitive Repair – Options
LIFT Procedure (Ligation of Intersphincteric Fistula Tract)
The intersphincteric space is opened (between internal and external sphincters) and the fistula tract is ligated (tied off) and divided at this point. Neither sphincter is divided. Sphincter-completely-sparing.
- Success rate: 60-80%
- Incontinence risk: Very low
- Best for: Transsphincteric fistulas after seton
- Recovery: 1-2 weeks
Mucosal Advancement Flap
A flap of rectal mucosa and submucosa is raised from inside the rectum and advanced to cover and close the internal opening of the fistula. The tract is curetted.
- Success rate: 60-80%
- Incontinence risk: Low
- Best for: Complex transsphincteric fistulas in patients with good sphincter function
- Technical note: Flap must be tension-free and well-vascularized technical demand is high
FiLaC Laser Closure
As a stage 2 procedure after seton, Laser Fistula Treatment Dubai may be used for simple or moderately complex fistulas.
- Success rate: 60-70%
Fistula Plug
A cone-shaped bioabsorbable plug (porcine small intestinal submucosa) is placed in the tract to promote ingrowth of new tissue.
- Success rate: 25-50% lowest of all options
- Advantage: No cutting, no incontinence risk
- Best used in: Patients for whom other options are too risky
Fibrin Glue
The fistula tract is cleaned and injected with fibrin glue (a biological sealant). Low success rate (25-40%) but minimal morbidity. May be combined with other techniques.
Long-Term Draining Seton
For Crohn’s fistulas or patients in whom cure is not achievable, a permanent draining seton provides quality of life by preventing recurrent abscesses. This is a palliation strategy, not a cure.
Complex Fistula with Crohn’s Disease
Crohn’s fistulas require a completely different approach:
- Medical treatment first: Biologics (infliximab, adalimumab) reduce inflammation and may close or simplify the fistula before surgery
- Surgery: Seton for drainage; definitive repair only in remission
- Stoma: Occasionally required to allow healing of a very complex Crohn’s fistula temporary or permanent
What to Expect: Realistic Outcomes
Complex fistula surgery is more challenging than simple fistula surgery. Patients should understand:
- Success rates are lower (60-80%) than for simple fistulas (>90%)
- More than one operation may be needed
- Some fistulas – particularly Crohn’s-related may never be fully cured with surgery alone
- The surgeon’s experience and correct technique selection significantly affect outcomes
Need expert treatment for hemorrhoids, anal fissure, or anal fistula? Book a consultation with Dr. Antonio Privitera in Dubai or Abu Dhabi.
📱 WhatsApp: +971 55 318 8469
📞 Phone: +971 55 318 8469
AUTHOR AUTHORITY BLOCK
Fellowship-trained at Mayo Clinic (USA) and the Royal College of Surgeons (UK). Member of the Royal College of Surgeons of Edinburgh. Certified in General Surgery by the Italian Medical Council.
About the Author
