
After being told you need an MRI for an anal fistula, most patients ask the same question: ‘Why? Can’t the surgeon just see it?’ The answer is that while the external opening of a fistula is visible, the tract the tunnel can be very complex, with branches, secondary tracts, and involvement of sphincter muscles that cannot be assessed by examination alone. Our anal fistula treatment in Dubai explains how imaging guides surgical planning. MRI is the only investigation that maps this anatomy reliably.
What MRI Shows
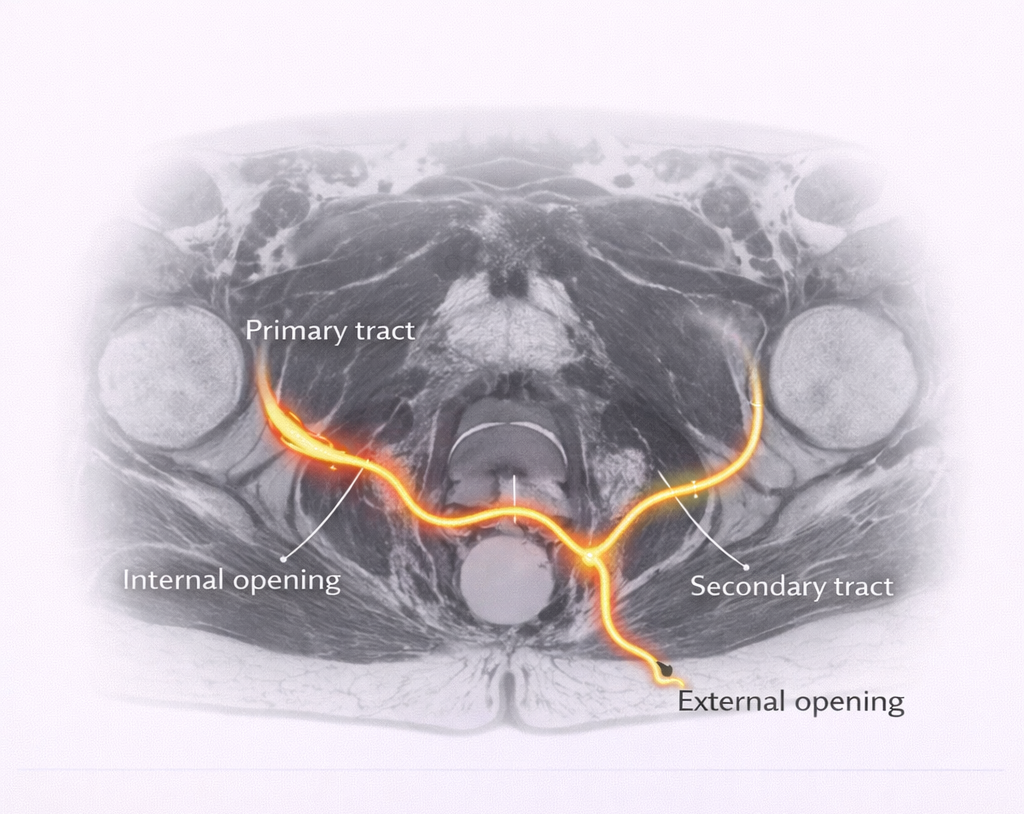
- Primary tract: The main tunnel from the internal opening to the external opening its exact path through or around the sphincter muscles
- Secondary tracts: Extensions or branches of the main tract horseshoe extensions, upward extensions, collections
- Internal opening: The location where the fistula connects to the anal canal essential for surgical planning
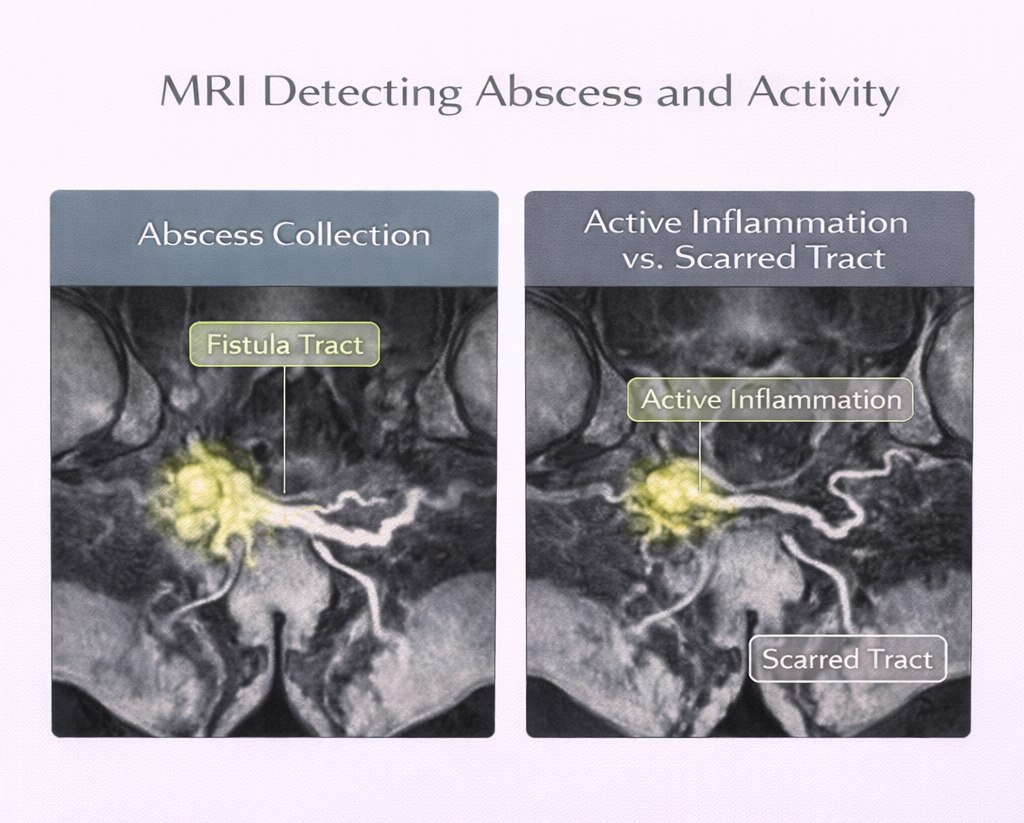
- Abscesses: Any residual collections that need to be drained before or during fistula repair
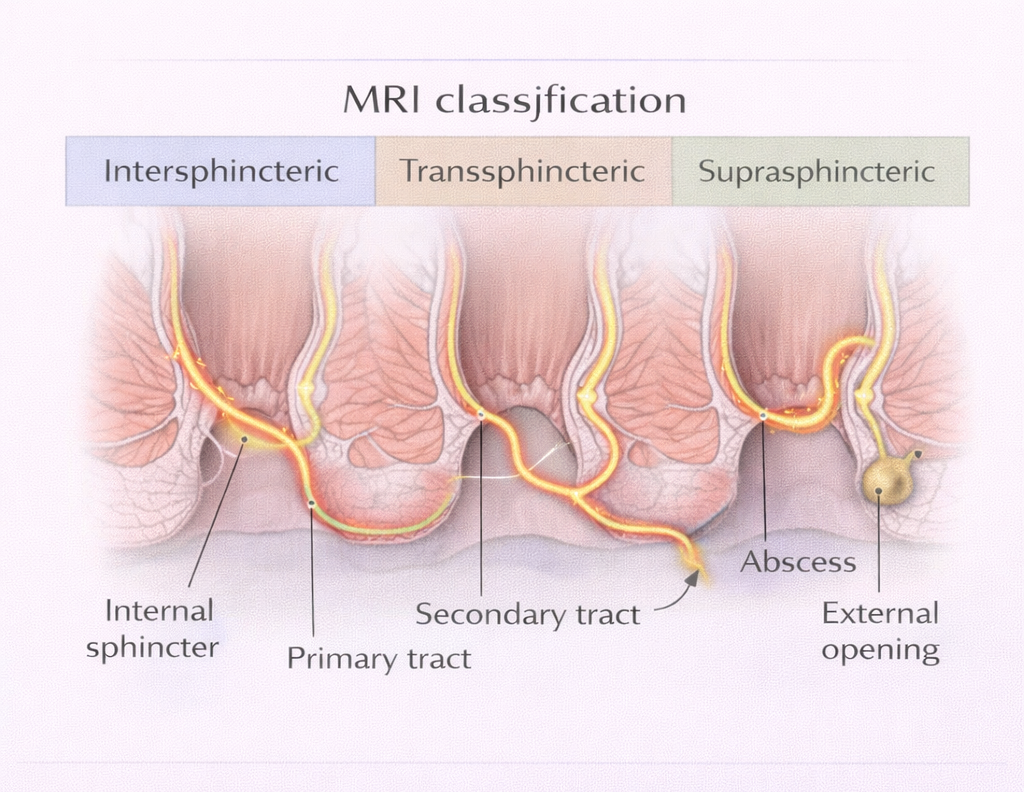
- Relation to sphincter: How much sphincter muscle is involved this determines whether a simple laying-open operation is safe or whether a sphincter-sparing technique is required
- Activity: MRI can show active inflammation vs. inactive/scarred tract important for timing of surgery
Why MRI Changes Surgical Planning
Identifying Secondary Tracts
Clinical examination may identify the primary tract. It will miss secondary tracts. In complex fistulas, secondary tracts that are not addressed at surgery will result in recurrence. Studies show that MRI identifies additional findings that change surgical management in 10–30% of cases.
Determining Sphincter Involvement
Sphincter involvement determines the surgical technique:
- No or minimal sphincter involvement → fistulotomy is safe
- Significant sphincter involvement → seton, LIFT, laser, or advancement flap required
Getting this wrong – laying open a high transsphincteric fistula – causes fecal incontinence. MRI prevents this error.
Detecting Unsuspected Crohn’s Disease
MRI findings that suggest Crohn’s fistula (multiple tracts, cavitating lesions, thickened bowel wall) prompt further investigation endoscopy, biopsies that change management completely. Complex cases differ. See complex fistula treatment.
When Is MRI Required?
- Complex fistula: Multiple external openings, previous failed surgery, long-standing or recurrent fistula
- Any fistula before definitive surgery (some surgeons perform MRI routinely some selectively)
- Suspected Crohn’s-related fistula
- Recurrent fistula after previous repair
- Fistula in which the internal opening cannot be identified clinically
When Is MRI NOT Required?
Simple, low intersphincteric fistulas with clear anatomy particularly in a patient with no previous surgery and a single external opening can sometimes be managed without preoperative MRI if the surgeon is confident of the anatomy after examination under anesthesia. This is a clinical decision.
The MRI Protocol
Not all MRI scans are equally useful for fistula. The correct protocol is:
- High-resolution MRI pelvis with dedicated anal fistula sequences
- T2-weighted and fat-suppression (STIR) sequences
- Thin slice through the anal canal
- Preferably read by a radiologist with experience in pelvic floor and colorectal imaging
In Dubai, this study is available at most major hospitals and diagnostic centers.
Need expert treatment for hemorrhoids, anal fissure, or anal fistula? Book a consultation with Dr. Antonio Privitera in Dubai or Abu Dhabi.
📱 WhatsApp: +971 55 318 8469
📞 Phone: +971 55 318 8469
AUTHOR AUTHORITY BLOCK
Fellowship-trained at Mayo Clinic (USA) and the Royal College of Surgeons (UK). Member of the Royal College of Surgeons of Edinburgh. Certified in General Surgery by the Italian Medical Council.
About the Author
