
Most anal fistulas are caused by a single, specific mechanism: infection of an anal gland. Understanding this mechanism helps explain why fistulas form, why they do not heal on their own, and why the right surgical approach is so important. For full management, see anal fistula treatment in Dubai.
The Primary Cause: Cryptoglandular Infection
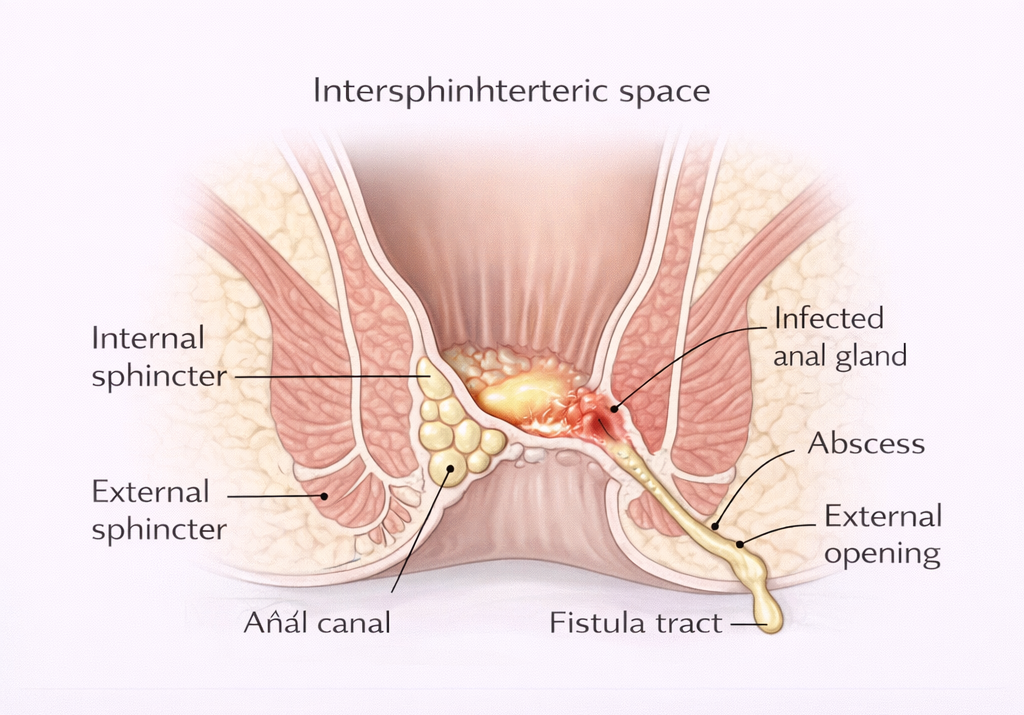
The anal canal has 6-10 small glands (anal cryptoglands) located in the intersphincteric space between the internal and external sphincters. These glands can become blocked and infected, resulting in an anal abscess.
If that abscess:
- Is surgically drained: A wound is created that may leave a persistent tract
- Drains spontaneously: The pus finds its own way to the skin surface, creating a natural fistula
In approximately 50% of perianal abscesses, a fistula tract remains after the acute infection resolves. The tract is lined by granulation tissue or epithelium and does not close spontaneously. Most fistulas arise after abscess formation. See fistula vs abscess.
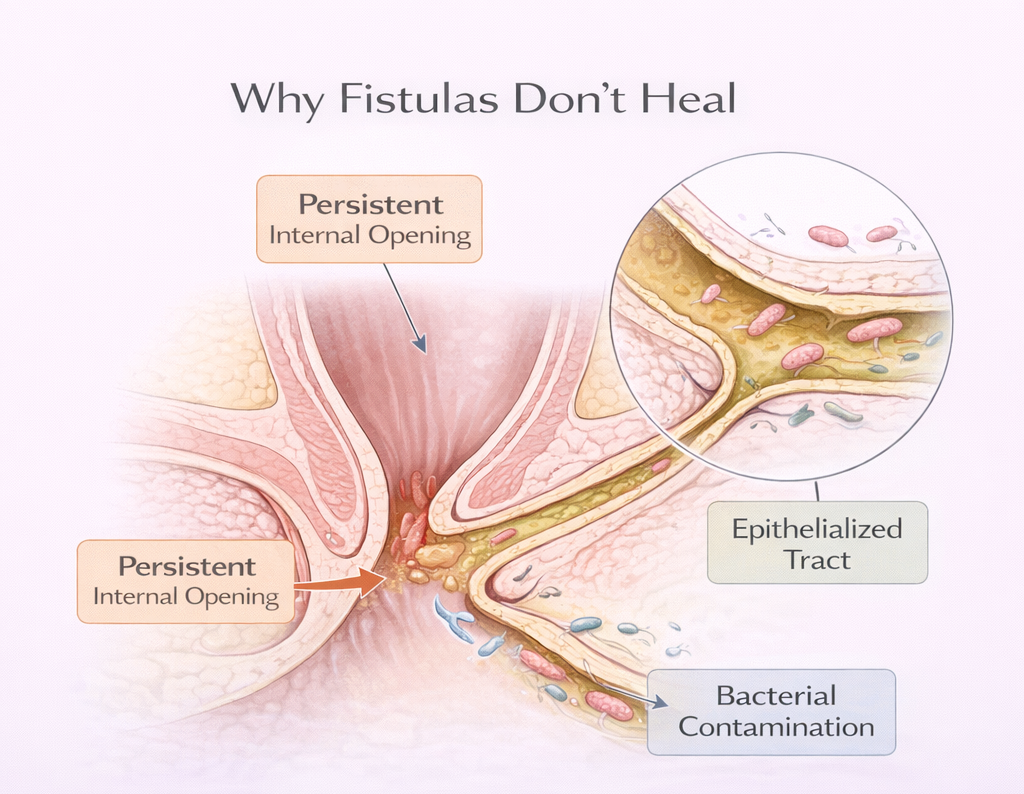
Why Fistulas Don’t Heal on Their Own
- The internal opening at the infected gland persists as a source of re-infection
- The tract is lined by tissue that actively prevents it from closing
- Fecal material and bacteria can enter the tract from the anal canal, perpetuating infection
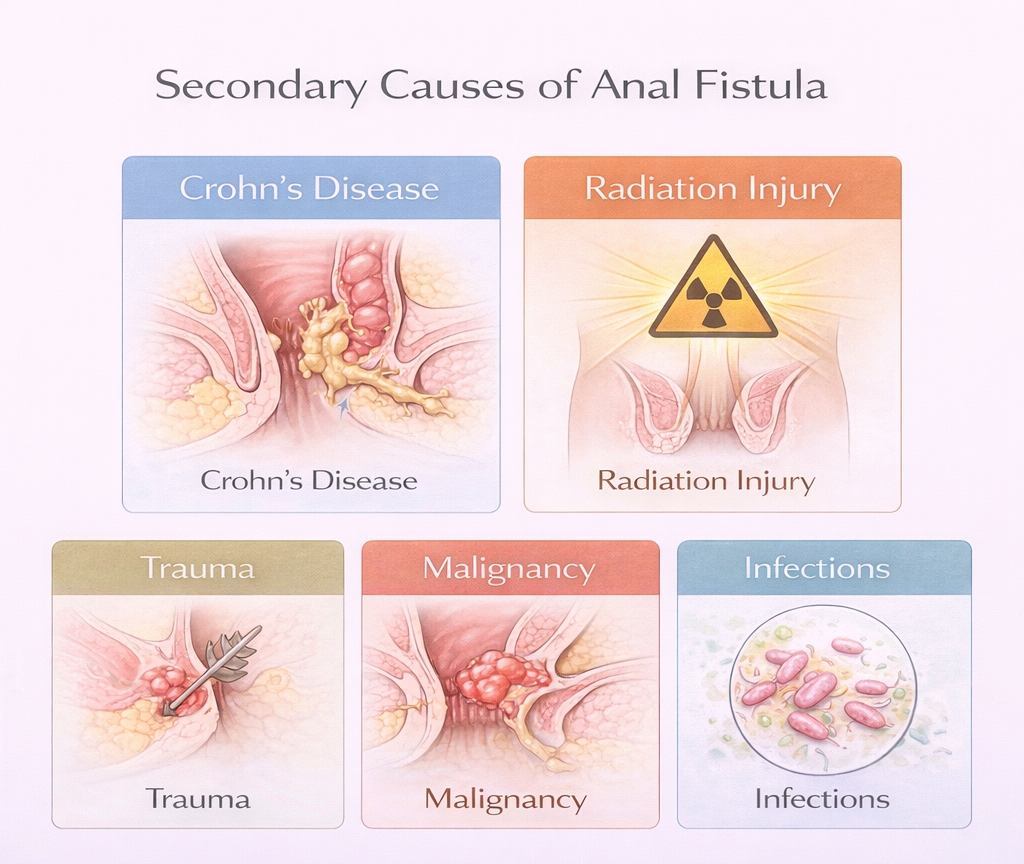
Secondary Causes
Crohn’s Disease
Crohn’s disease anal fistulas in Dubai cause transmural inflammation of the GI tract. In the perianal area, this leads to:
- Complex fistulas – often multiple tracts, multiple external openings, extensive involvement of sphincter and surrounding tissue
- Atypical fistulas – broad-based, cavitating, poorly healing
- High recurrence rate even after surgery Any patient with a complex or atypical fistula, multiple fistulas, or fistula with poor healing should be investigated for Crohn’s disease.
Radiation Injury
Pelvic radiotherapy (for prostate, cervical, rectal, or bladder cancer) can damage the rectum and anal canal, leading to radiation proctitis and eventually fistula formation. These are complex fistulas with poor tissue quality and limited treatment options.
Trauma
Penetrating perianal injury, obstetric trauma (third or fourth degree perineal tears), or impalement injuries can create direct fistula tracts.
Malignancy
Anal, rectal, or vaginal cancers can infiltrate surrounding tissue and create fistula-like tracts. Important: Any fistula with atypical features (hard indurated tract, rapidly changing symptoms, associated mass) must be biopsied.
Tuberculosis
Anorectal TB is uncommon in UAE but should be considered in high-risk patients. Typically presents with multiple tracts, indolent healing, and constitutional symptoms.
Sexually Transmitted Infections
Lymphogranuloma venereum (LGV) and certain other STIs can cause perianal inflammation and fistula formation.
Risk Factors for Developing a Fistula After Abscess
- Young age at first abscess
- Male sex (cryptoglandular fistula is more common in men)
- Deep intersphincteric or ischiorectal abscesses (compared to subcutaneous)
- Inadequate drainage of the original abscess
References
- Parks AG, Gordon PH, Hardcastle JD. A classification of fistula-in-ano. Br J Surg. 1976.
- Whiteford MH. Perianal abscess/fistula disease. Clin Colon Rectal Surg. 2007.
Need expert treatment for hemorrhoids, anal fissure, or anal fistula? Book a consultation with Dr. Antonio Privitera in Dubai or Abu Dhabi.
📱 WhatsApp: +971 55 318 8469
📞 Phone: +971 55 318 8469
AUTHOR AUTHORITY BLOCK
Fellowship-trained at Mayo Clinic (USA) and the Royal College of Surgeons (UK). Member of the Royal College of Surgeons of Edinburgh. Certified in General Surgery by the Italian Medical Council.
About the Author
