
Yes – anal fistulas can recur after surgery. Recurrence is one of the most frustrating aspects of fistula treatment, particularly for complex fistulas. For full management, see anal fistula treatment in Dubai. Understanding why fistulas recur – and what can be done about it – helps set realistic expectations and guides treatment planning.
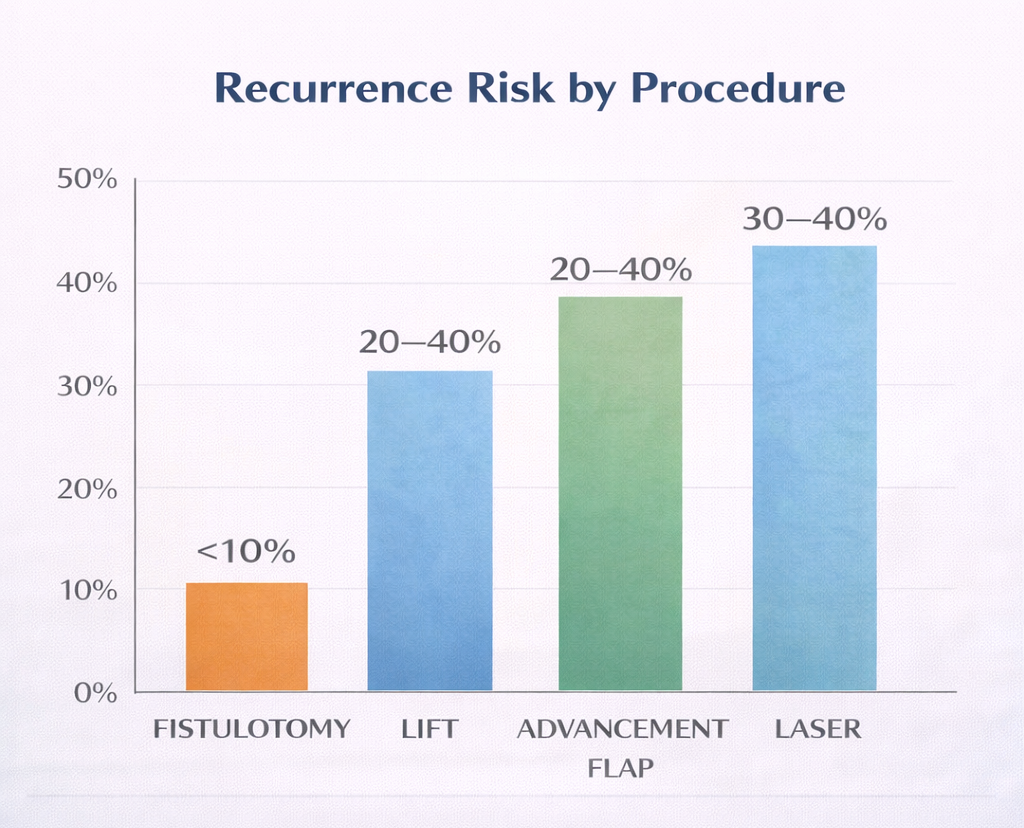
Recurrence Rates by Procedure
Fistulotomy
- Recurrence rate: Less than 10% for simple fistulas
- Cause of recurrence: Missed secondary tract or internal opening; inadequate laying open
- Management: Re-examination under anesthesia ± MRI; repeatfistulotomy if appropriate
LIFT Procedure
- Recurrence rate: 20-40%
- Cause: Residual tract in the ischiorectal side of the fistula; missed secondary tracts; technical failure of ligation
- Management: MRI; repeat LIFT, advancement flap, or conversion to seton if recurrence with persistent sepsis
Advancement Flap
- Recurrence rate: 20-40%
- Cause: Flap breakdown, persistent internal opening, inadequate curettage of tract
Laser (FiLaC)
- Recurrence rate: 30-40%
- Cause: Incomplete destruction of tract, missed internal opening
Why Fistulas Recurrence
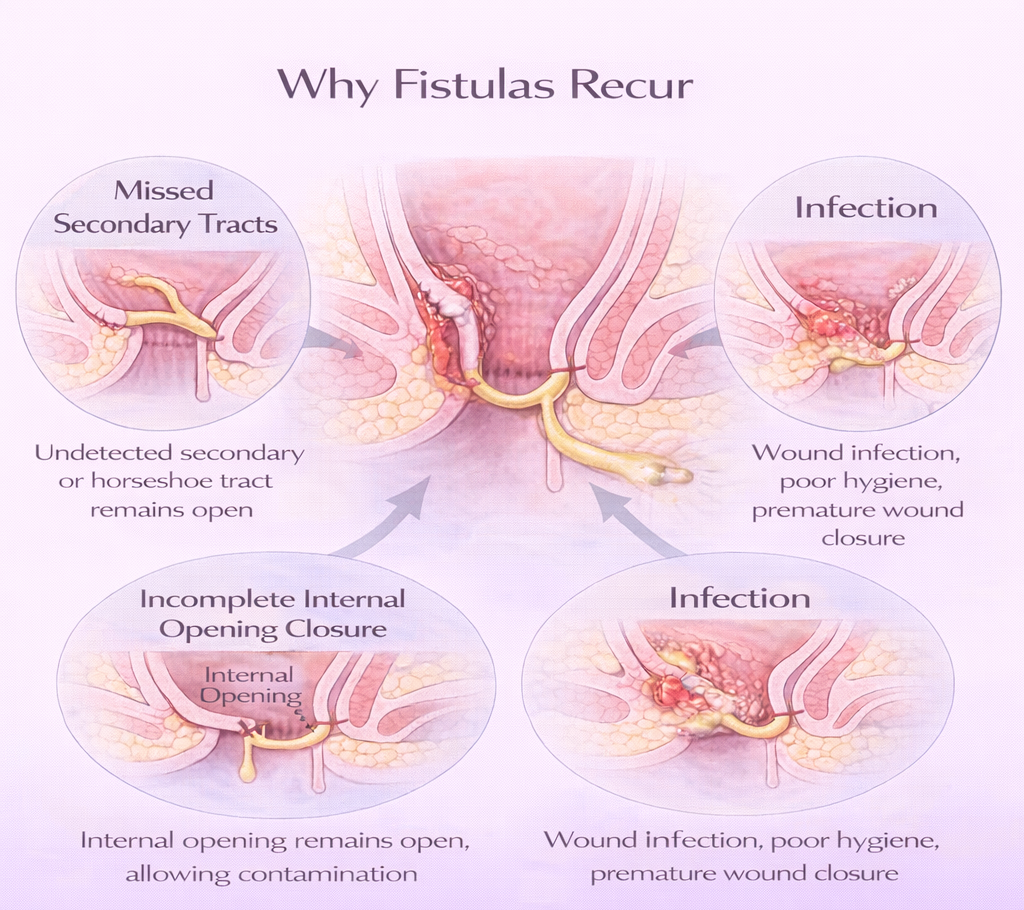
1. Missed Secondary Tract
The most common reason for recurrence after any fistula operation. If a secondary horseshoe tract or extension was not identified either because MRI was not performed or because the secondary tract was not accessible during surgery it remains patent and re-presents as recurrence.
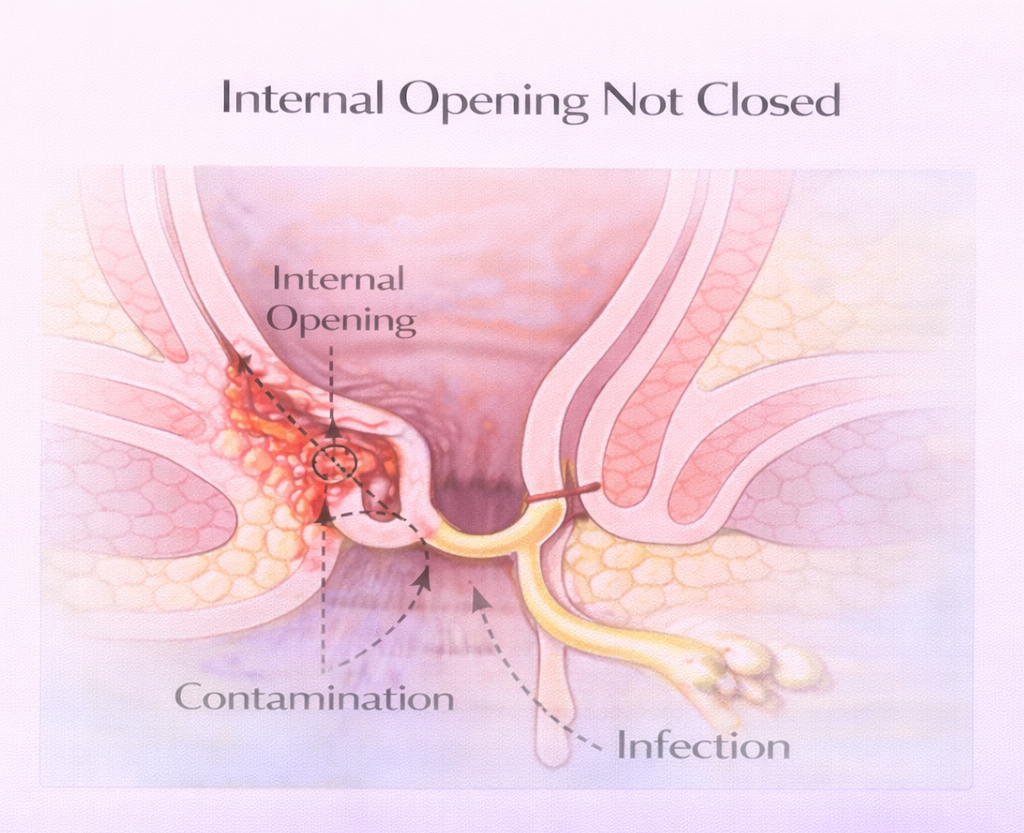
2. Incomplete Closure of Internal Opening
The internal opening (inside the anal canal) is the source. If it is not definitively closed, the source of contamination persists, and the tract reforms.
3. Crohn’s Disease
Fistulas in Crohn’s disease recur at significantly higher rates than cryptoglandular fistulas, regardless of surgical technique. Medical treatment with biologics is essential to reduce recurrence.
4. Inadequate Postoperative Care
Wound infection, premature closure of the wound surface (sealing over before healing from the base), and poor hygiene all impair healing and increase recurrence risk.
What to Do If Your Fistula Has Come Back
- Do not panic – recurrence is treatable
- See a specialist promptly – early treatment of a recurrent fistula is much simpler than treating a long-standing recurrence with progressive sepsis
- MRI: Essential in recurrent fistula – the anatomy has changed from previous surgery, and examination alone is unreliable. See MRI for anal fistula.
- Ask whether you were treated by a specialist colorectal surgeon – recurrence rates are lower in experienced hands
Second Opinions After Failed Fistula Surgery
A second opinion for failed fistula surgery in Dubai is appropriate if your symptoms have returned, or never fully resolved. Management of recurrent fistula is complex and benefits from experience in the full range of sphincter-sparing techniques.
Need expert treatment for hemorrhoids, anal fissure, or anal fistula? Book a consultation with Dr. Antonio Privitera in Dubai or Abu Dhabi.
📱 WhatsApp: +971 55 318 8469
📞 Phone: +971 55 318 8469
AUTHOR AUTHORITY BLOCK
Fellowship-trained at Mayo Clinic (USA) and the Royal College of Surgeons (UK). Member of the Royal College of Surgeons of Edinburgh. Certified in General Surgery by the Italian Medical Council.
About the Author
