
A chronic anal fissure is not simply an acute fissure that has lasted longer. It is a fundamentally different clinical entity. Our anal fissure treatment in Dubai explains why chronic fissures develop and what the full treatment pathway looks like. The tissue changes, the treatment requirements change, and the risk of recurrence is higher unless the underlying cause is permanently addressed.
This guide explains exactly why chronic fissures don’t heal and what you need to do to resolve them once and for all.
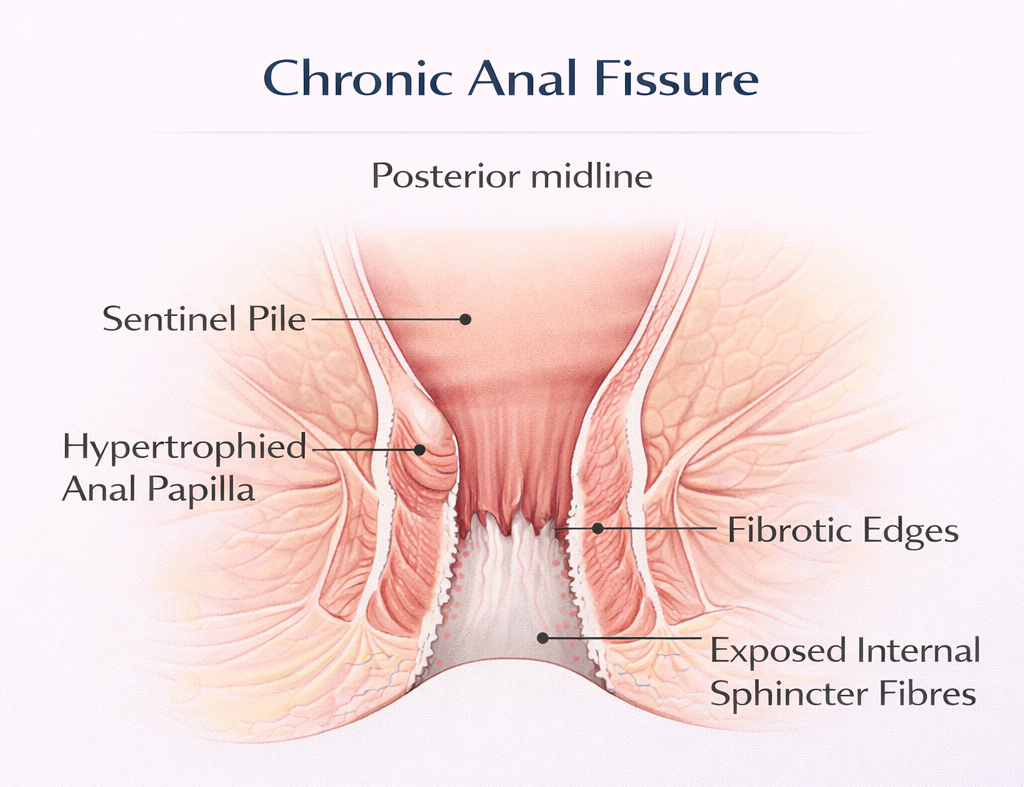
What Makes a Fissure ‘Chronic’?
- Duration: More than 6 weeks (some authorities use 8 weeks or 3 months)
- Structural changes: Development of a sentinel pile (skin tag at the outer edge), hypertrophied anal papilla (at the inner edge), and fibrotic, pale, deep edges that often expose the white fibres of the internal sphincter
- Failure to respond to simple measures: A chronic fissure will not heal with diet and cream alone if the cycle of spasm, ischemia, and fibrosis is already established
The Spasm-Ischemia Cycle: Why It Becomes Self-Perpetuating
Here is the core problem:
- Tear occurs → internal sphincter spasm
- Spasm reduces blood supply to posterior midline
- Poor blood supply means the tear cannot heal
- Persistent tear → ongoing sphincter stimulation → ongoing spasm
- Repeated cycles lead to fibrosis of the fissure edges
- Fibrotic edges cannot bridge the gap even if blood supply improves To break this cycle, you must address the spasm (creams, Botox, or surgery) AND optimize healing conditions (diet, hydration, soft stool).
Why Creams Often Fail for Chronic Fissures
GTN and diltiazem creams reduce sphincter pressure by 20-30%. For a moderately tight sphincter with a recent-onset fissure, this may be enough. For a very tight sphincter with a fully fibrotic chronic fissure, a 20-30% reduction is insufficient to restore adequate blood supply and overcome the structural barrier.
Treatment That Works for Chronic Fissures
Botox Injection
Botox Anal Fissure Dubai Preferred second-line treatment. Reduces sphincter pressure more profoundly than creams. Healing rate:
60-70%. Temporary effect the fissure can recur if the underlying cause (constipation) is not corrected.
Lateral Internal Sphincterotomy (LIS)
Lateral Internal Sphincterotomy Dubai The definitive treatment. Permanently reduces sphincter pressure. Healing rate 95%. Recurrence very rare. Reserved for fissures that fail Botox or present with very high sphincter pressure from the outset.
Why Fissures Come Back After Treatment
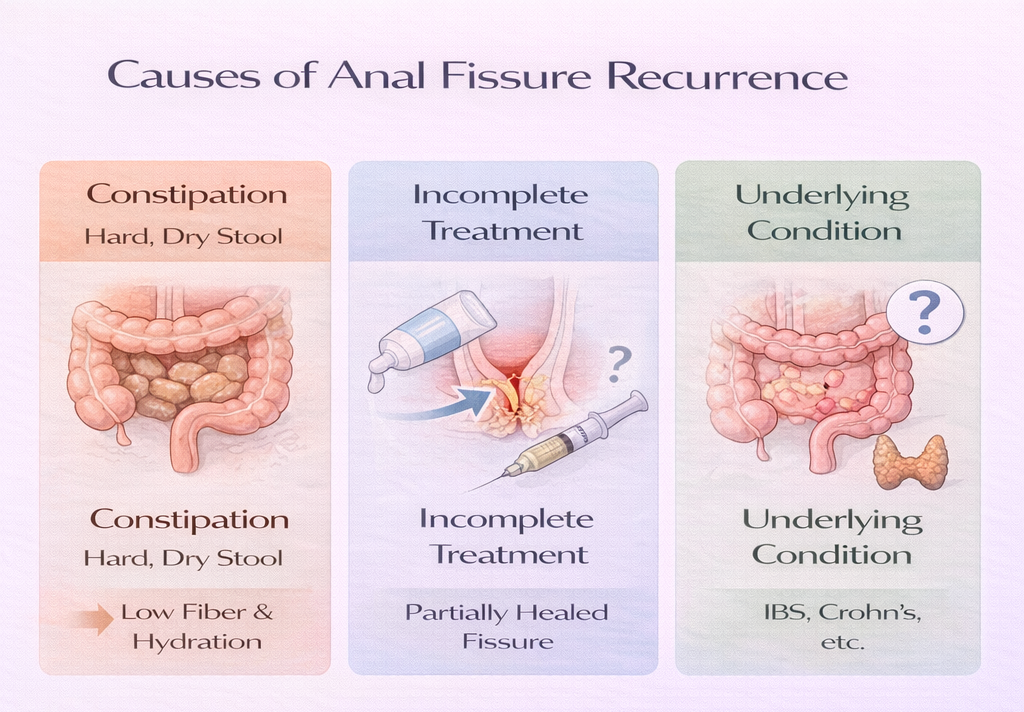
Most Common Reason: Constipation Returns
The dietary changes and stool softeners that supported healing during treatment must be maintained indefinitely. The sphincter may remain relatively tight even after a fissure heals a return to hard stools can re-tear the same weak area.
Incomplete Treatment
Stopping topical cream too early, or not following through with Botox after cream failure, leaves a partially healed fissure that re-opens easily.
Underlying Conditions
Crohn’s disease, IBS with constipation, hypothyroidism, and other conditions that chronically affect bowel function will perpetuate fissure recurrence if not treated.
Long-Term Management: Preventing Recurrence
- High-fiber diet permanently – not just during treatment
- Adequate hydration – 2.5-3 liters daily in UAE climate
- Regular physical activity to support bowel motility
- Prompt treatment of any constipation episode with stool softeners
- Follow-up if symptoms return – early treatment of a new acute fissure prevents it becoming chronic again
Need expert treatment for hemorrhoids, anal fissure, or anal fistula? Book a consultation with Dr. Antonio Privitera in Dubai or Abu Dhabi.
📱 WhatsApp: +971 55 318 8469
📞 Phone: +971 55 318 8469
AUTHOR AUTHORITY BLOCK
Fellowship-trained at Mayo Clinic (USA) and the Royal College of Surgeons (UK). Member of the Royal College of Surgeons of Edinburgh. Certified in General Surgery by the Italian Medical Council.
About the Author
