
Anal fissure and anal fistula sound similar and both affect the perianal area, but they are completely different conditions. However, they have different causes, different examinations, and completely different treatments. For a complete overview of anal fissure diagnosis and treatment, see anal fissure treatment in Dubai. Confusing them, or treating one when you have the other, will not work.
This guide explains both conditions clearly so you know what you are dealing with.
What Is an Anal Fissure?
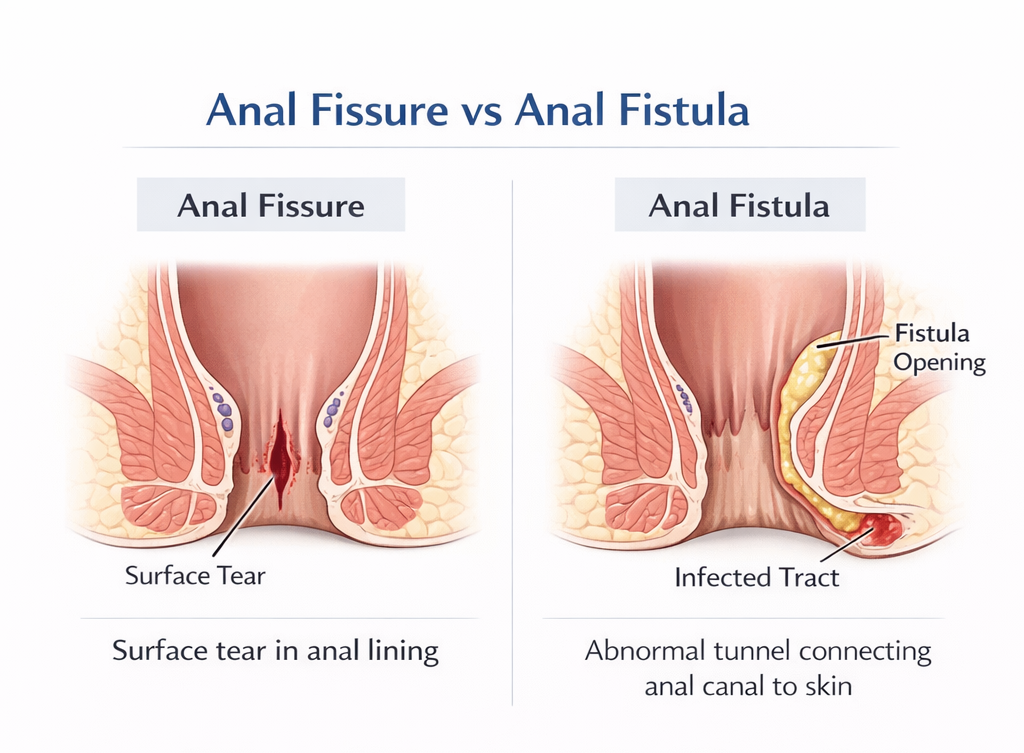
An anal fissure is a tear in the lining of the anal canal – the short passage between the rectum and the outside. It is a surface injury. There is no tunnel, no abscess, no opening on the skin.
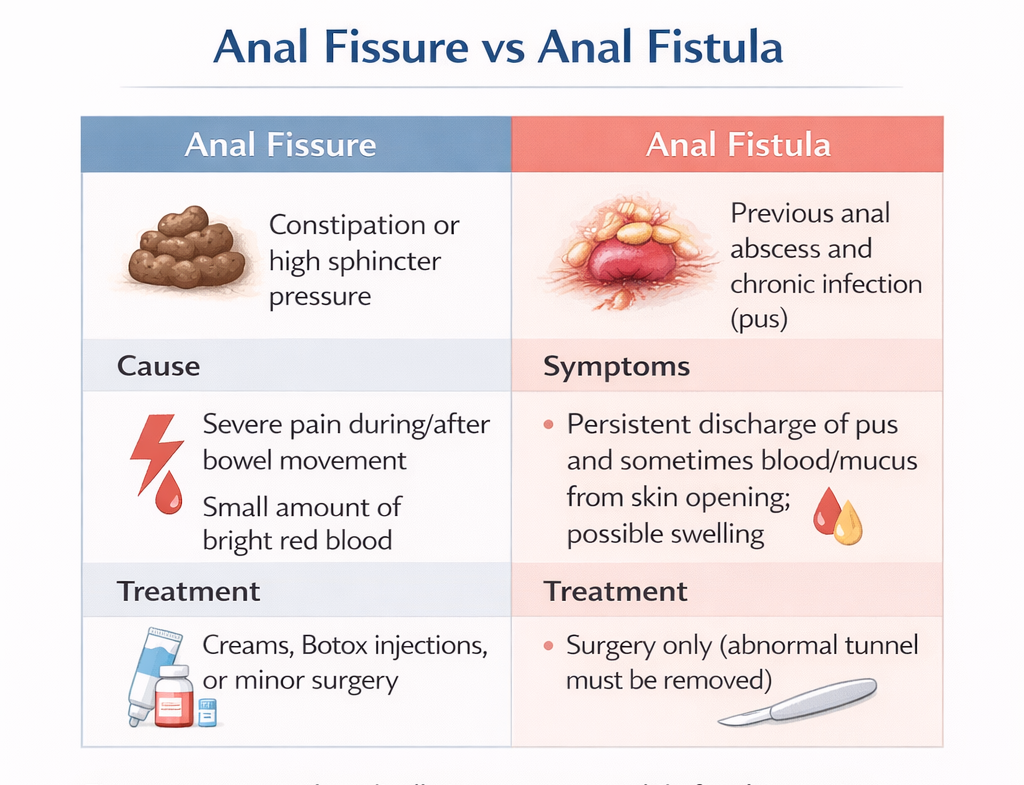
- Cause: Stretching of the anal canal by hard stool; chronic constipation; high sphincter pressure.
- Appearance: A crack or split in the anal lining, usually at the posterior midline (6 o’clock).
- Key symptoms: Sharp pain during and after bowel movements, lasting 30–90 minutes; small amount of bright red blood.
- Treatment: Dietary changes, topical creams (GTN, diltiazem), Botox, or surgery (LIS) in resistant cases.
What Is an Anal Fistula?
An anal fistula is an abnormal tunnel connecting the inside of the anal canal to the skin around the anus. For full management options, see anal fistula treatment in Dubai. It is not a surface injury – it is a tract that passes through or around the sphincter muscles.
- Cause: Almost always a previous anal abscess (infection of an anal gland) that drained – either spontaneously or surgically – and left a persistent tunnel.
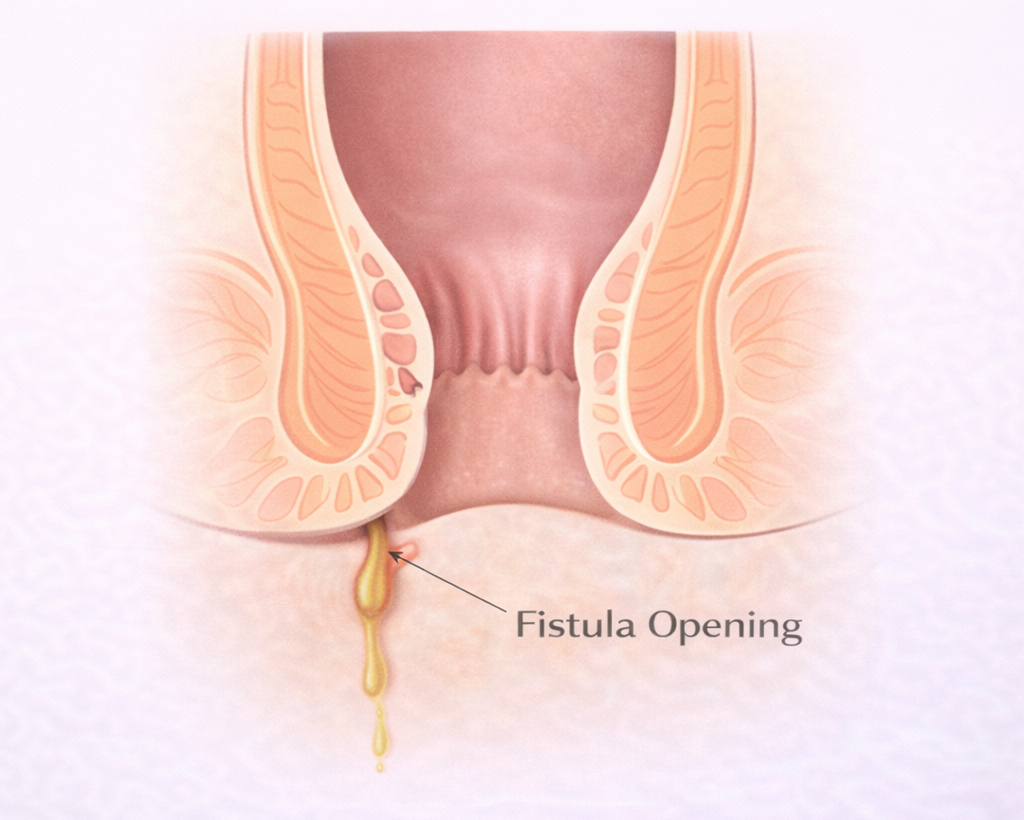
- Appearance: A visible external opening (fistula opening) on the skin near the anus, sometimes with discharge.
- Key symptoms: Persistent discharge (pus, blood, mucus) from an opening near the anus; may have itching, discomfort, or intermittent swelling. Less likely to cause the severe pain-after-bowel-movement pattern of a fissure.
- Treatment: Surgical – the fistula tract must be laid open or otherwise obliterated. It will NOT heal on its own and cannot be treated with creams.
Side-by-Side Comparison
- Anal Fissure: Surface tear in anal lining. Pain during/after bowel movement. Small amount of blood. No external opening. Treatment: creams / Botox / LIS.
- Anal Fistula: Tunnel from inside anal canal to perianal skin. Persistent discharge from external opening. Less pain than fissure unless abscess develops. Treatment: surgery only.
Can You Have Both?
Yes. Patients with Crohn’s disease frequently have both fissures and fistulas simultaneously. Chronic fissures can also coexist with internal openings that technically qualify as very shallow fistulas. This is another reason why examination by a colorectal surgeon not self-diagnosis is essential. Pain patterns differ. See anal pain causes.
Key Question: Which One Do You Have?
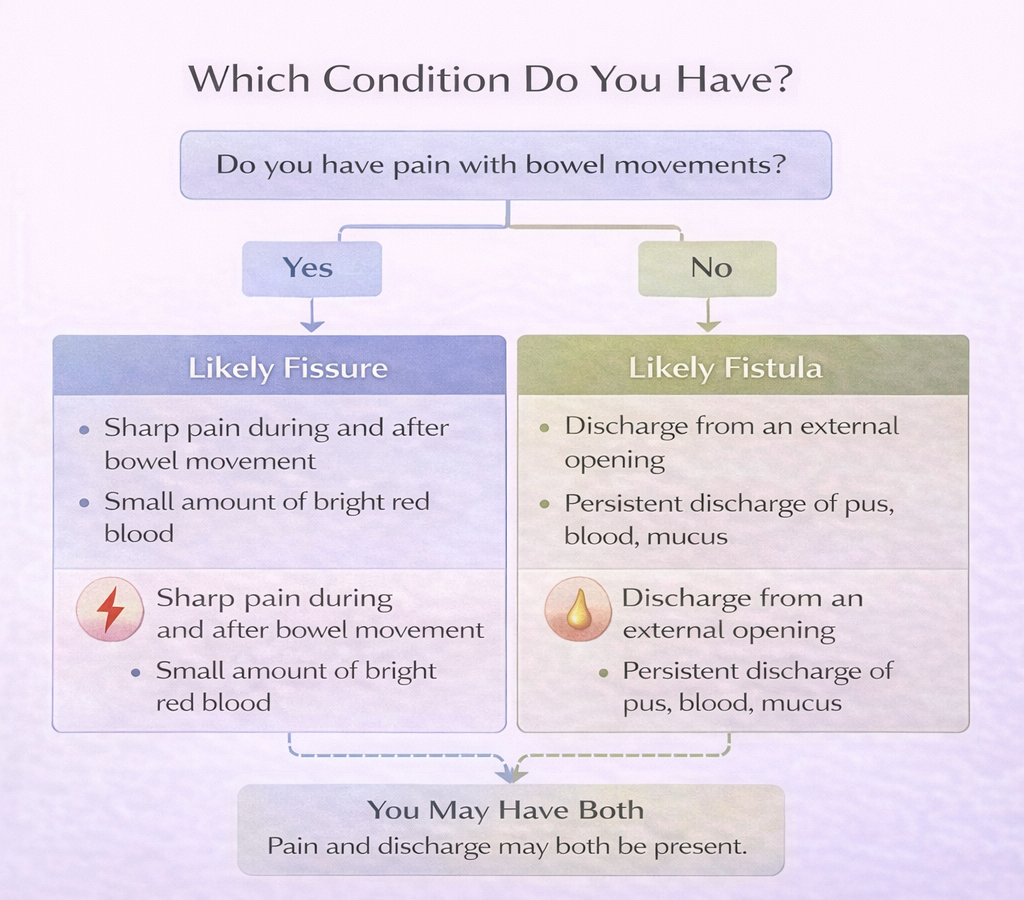
- Do you have an external opening or hole near your anus with discharge? → Likely fistula.
- Do you have severe pain during and after every bowel movement with a small amount of blood? → Likely fissure.
- Do you have both? → Both conditions may be present – specialist evaluation required.
References
- Whiteford MH. Perianal abscess/fistula disease. Clin Colon Rectal Surg. 2007.
- Steele SR et al. Practice parameters for the management of perianal abscess and fistula-in-ano. Dis Colon Rectum. 2011.
Need expert treatment for hemorrhoids, anal fissure, or anal fistula? Book a consultation with Dr. Antonio Privitera in Dubai or Abu Dhabi.
📱 WhatsApp: +971 55 318 8469
📞 Phone: +971 55 318 8469
AUTHOR AUTHORITY BLOCK
Fellowship-trained at Mayo Clinic (USA) and the Royal College of Surgeons (UK). Member of the Royal College of Surgeons of Edinburgh. Certified in General Surgery by the Italian Medical Council.
About the Author
