
Table of Contents
Hemorrhoids (Piles) Treatment in Abu Dhabi
If you’re dealing with hemorrhoid symptoms — bleeding during bowel movements, a persistent lump you can feel, itching, or discomfort — you’re not alone, and effective hemorrhoid treatment in Abu Dhabi is available. I’m Professor Dr. Antonio Privitera, a consultant colorectal surgeon with fellowship training at the Mayo Clinic and in London, and European Board Certification in Colorectal Surgery. I specialize in the diagnosis and treatment of hemorrhoids and other anorectal conditions.
In my practice, I see patients every day who’ve delayed seeking care because of embarrassment or fear of surgery. The truth is straightforward: most hemorrhoids don’t require surgery, and when they do, modern techniques have dramatically reduced pain and recovery time.
What matters most is accurate diagnosis, because not all rectal bleeding or discomfort is caused by hemorrhoids, and choosing treatment based on the grade and type of hemorrhoid you have, not marketing claims.
Here’s what sets our approach apart:
- Accurate diagnosis first: We examine you properly (visual inspection, digital exam, anoscopy when needed) to confirm hemorrhoids and rule out other causes of your symptoms — including fissures, fistulas, polyps, or colorectal cancer.
- Grade-based treatment: A Grade 1 internal hemorrhoid responds well to dietary changes; a Grade 4 prolapsed hemorrhoid usually needs surgery. We match the treatment to your condition, not the other way around.
- Discreet, same-day assessment available: Privacy matters. We offer consultations at multiple locations across Abu Dhabi with flexible scheduling and complete confidentiality.
This guide explains everything you need to know about hemorrhoid treatment in Abu Dhabi, from symptoms and diagnosis to the full range of treatment options available.
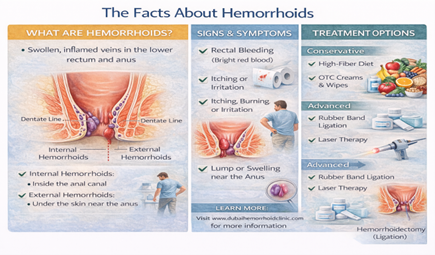
What Are Hemorrhoids?
Hemorrhoids (also called piles) are swollen blood vessels in the lower rectum and anal canal. Everyone has hemorrhoidal tissue — these vascular cushions help with continence and sensation. Hemorrhoids become a problem when they enlarge, bleed, prolapse (come out of the anus), or cause pain.
There are two types:
- Internal hemorrhoids sit inside the rectum, above the dentate line (the boundary between rectal tissue and anal skin). You usually can’t see or feel them. They’re covered by rectal mucosa, which has no pain receptors, so internal hemorrhoids typically don’t hurt — they bleed.
- External hemorrhoids are under the skin around the anus, below the dentate line. Because this area has pain receptors, external hemorrhoids can be painful, especially if a clot forms inside them (thrombosed external hemorrhoid).
Hemorrhoids are extremely common, with many adults experiencing symptoms at some point in their lives, particularly between ages 45 and 65, though I regularly see patients in their 20s and 30s as well — especially in Abu Dhabi’s office-working, sedentary population.
Symptoms of Hemorrhoids: What You Might Notice
Hemorrhoid symptoms vary depending on whether they’re internal or external, and what grade they are. Here’s what patients typically experience:
Bleeding
Bright red blood on toilet paper, in the toilet bowl, or on the surface of stool. This is the most common symptom of internal hemorrhoids. The bleeding is usually painless and happens during or just after a bowel movement. If you see blood, it’s important to get checked — while hemorrhoids are a common cause of rectal bleeding, other conditions (fissures, polyps, inflammatory bowel disease, cancer) can also cause bleeding.
A lump or swelling
You might feel a soft lump near your anus. This could be a prolapsed internal hemorrhoid (one that’s come out through the anus) or an external hemorrhoid. If the lump appeared suddenly and is painful, it may be a thrombosed external hemorrhoid (a clot inside).
Itching or irritation
Mucus discharge from prolapsing internal hemorrhoids can irritate the anal skin, causing itching (pruritus ani). Moisture and poor cleaning can make this worse.
Discomfort or pain
Internal hemorrhoids usually don’t hurt unless they prolapse and become strangulated (blood supply is cut off). External hemorrhoids can be uncomfortable, and thrombosed external hemorrhoids are often very painful for the first 48–72 hours.
Mucus discharge or soiling
When internal hemorrhoids prolapse, they can leak mucus, leading to a feeling of dampness and sometimes minor staining of underwear.
A feeling of incomplete evacuation
Large internal hemorrhoids can make you feel like you haven’t fully emptied your bowels.
When symptoms mean something more serious:
If you experience heavy bleeding, severe pain with fever, sudden weakness or dizziness, significant weight loss, or a change in bowel habits (new constipation or diarrhea lasting more than a few weeks), you need urgent evaluation. These can be signs of other conditions that require immediate attention.
It’s Not Always Hemorrhoids: What Else Could It Be?
This is one of the most important parts of my role as a colorectal surgeon: not assuming that rectal bleeding or anal discomfort is automatically hemorrhoids. I’ve seen too many patients who were told they had hemorrhoids based on symptoms alone, without proper examination.
Here are other conditions that can cause similar symptoms:
Anal fissure
A tear in the anal lining, usually caused by passing hard stool.
Fissures cause sharp pain during and after bowel movements, and you may see a small amount of bright red blood. Unlike hemorrhoids, fissures hurt significantly.
Anal fistula
An abnormal tunnel between the inside of the anal canal and the skin near the anus, usually resulting from an infection (abscess). Fistulas cause discharge (pus, blood, or mucus), irritation, and sometimes pain.
They don’t resolve on their own and require treatment.
Anal abscess
A collection of pus near the anus, causing severe pain, swelling, fever, and difficulty sitting. This is a surgical emergency.
Polyps or colorectal cancer
Polyps (growths on the colon lining) and cancer can both cause rectal bleeding. The blood may be darker (maroon or mixed with stool) or bright red. This is why screening matters, especially after age 40 in the UAE.
Inflammatory bowel disease (IBD)
Conditions like Crohn’s disease or ulcerative colitis cause bleeding, diarrhea, abdominal pain, and weight loss. These require very different treatment from hemorrhoids.
Rectal prolapse
The rectum itself protrudes through the anus (different from a prolapsed hemorrhoid). This usually requires surgical repair.
This is why examination matters. A proper assessment includes a visual inspection, a digital rectal exam, and often anoscopy (a small scope to look inside the anal canal). If there are any red flags — your age, family history, blood mixed with stool rather than separate, weight loss — I’ll recommend colonoscopy to examine the entire colon.
Red Flags: When You Need Urgent Evaluation
Most hemorrhoid symptoms are not dangerous, but certain signs should prompt you to seek medical care quickly:
- Heavy bleeding that soaks through toilet paper or causes clots in the toilet
- Bleeding with dizziness, weakness, or fainting (possible anemia)
- Severe, constant pain (not just discomfort during bowel movements)
- Fever with anal pain or swelling (possible abscess)
- Significant, unexplained weight loss (more than 5 kg in a few months)
- Change in bowel habits lasting more than 2–3 weeks (new constipation, diarrhea, or narrowing of stool)
- Blood that’s dark, maroon, or mixed throughout the stool (rather than bright red on the surface)
- Any rectal bleeding if you’re over 40 and haven’t been screened for colon cancer
In the UAE, colorectal cancer screening typically starts at age 40, earlier than in some other countries. This reflects both local population demographics and alignment with international guidelines from the Abu Dhabi Department of Health and Cleveland Clinic Abu Dhabi. If you’re 40 or older and experiencing any rectal bleeding — even if you’re certain it’s hemorrhoids — it’s important to undergo colon screening (usually colonoscopy) to rule out polyps or cancer. Early detection of colorectal cancer is highly treatable.
Internal vs External Hemorrhoids: Why the Difference Matters
Understanding whether your hemorrhoids are internal or external helps explain your symptoms and guides treatment.
Internal Hemorrhoids
- Located inside the rectum, above the dentate line
- Covered by rectal mucosa (no pain receptors)
- Symptoms: Usually painless bleeding (bright red blood), possible prolapse (coming out of the anus), mucus discharge
- Treatment response: Respond well to rubber band ligation, sclerotherapy, infrared coagulation (for Grades I–II), and procedures like THD or laser (for Grades II–III)
External Hemorrhoids
- Located under the skin around the anus, below the dentate line
- Covered by skin (has pain receptors)
- Symptoms: Usually painless unless thrombosed (clotted), visible and palpable lumps, swelling, itching
- Treatment response: Conservative care for most; thrombosed ones may benefit from excision within 48–72 hours; large skin tags often removed surgically
Mixed Hemorrhoids
Many patients have both internal and external components. This is common in Grade III and IV hemorrhoids.
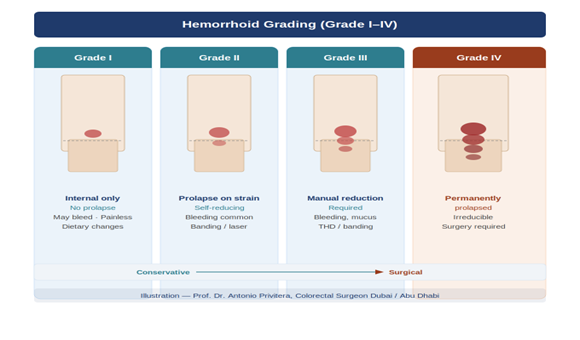
Hemorrhoid Grading System: Why It Changes Everything
The grade of your internal hemorrhoids determines which treatment is most likely to work. Grading is based on how much the hemorrhoid prolapses (comes out of the anus) and whether it goes back in on its own.
Grade I
Hemorrhoids bleed but don’t prolapse (don’t come out)
- You can’t see or feel them
- Typical treatment: Dietary changes, fiber, hydration, topical treatments; office procedures like rubber band ligation if bleeding persists
Grade II
Hemorrhoids prolapse during straining or bowel movements but go back inside on their own
- You might feel them briefly but they disappear
- Typical treatment: Rubber band ligation, sclerotherapy, infrared coagulation; sometimes laser or THD for larger Grade II
Grade III
Hemorrhoids prolapse and require manual reduction (you have to push them back in with your finger)
- They don’t stay inside on their own after a bowel movement
- Typical treatment: THD/HAL-RAR, laser hemorrhoidoplasty, or hemorrhoidectomy (surgery), depending on size and anatomy
Grade IV
Hemorrhoids are permanently prolapsed and cannot be pushed back inside
- They stay outside all the time
- Typical treatment: Usually hemorrhoidectomy (surgical removal); occasionally THD if there’s minimal external component
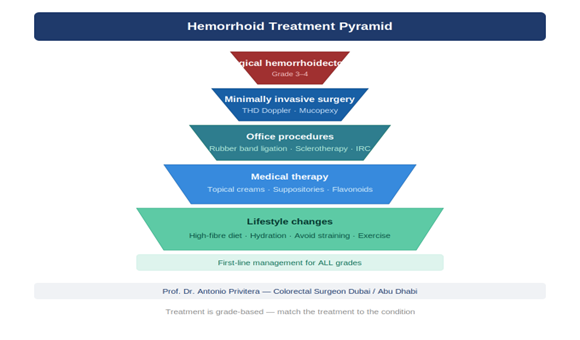
Why grading matters:
Different treatments work for different grades. It’s important to understand that treatment should be matched to your specific anatomy and grade. A Grade IV hemorrhoid typically requires surgical excision, while a Grade I hemorrhoid often responds to conservative measures. The safest approach is grade-based treatment selection, not a one-size-fits-all technique.
What Causes Hemorrhoids? (And Abu Dhabi-Specific Risk Factors)
Hemorrhoids develop when there’s increased pressure on the blood vessels in the rectum and anus. Common causes include:
Straining during bowel movements
Chronic constipation and hard stools are among the most common culprits. When you strain, you increase pressure in the abdomen and pelvis, which engorges hemorrhoidal vessels.
Prolonged sitting
Sitting for long periods — especially on the toilet — increases pressure on anal veins. In Abu Dhabi, I see this frequently in office workers who sit 10–12 hours a day in air-conditioned environments.
Chronic diarrhea
Repeated diarrhea irritates the anus and increases pressure.
Low-fiber diet
A diet low in fiber leads to hard stools and straining. Many expatriates in the UAE eat less fiber than they did in their home countries.
Dehydration
Abu Dhabi’s heat and air conditioning can lead to dehydration, making stools harder. If you’re not drinking enough water — especially in summer — you’re at higher risk.
Pregnancy and childbirth
The growing uterus increases pressure on pelvic veins, and straining during delivery can cause or worsen hemorrhoids. Hormonal changes also relax vein walls.
Aging
The tissues supporting hemorrhoids weaken with age. Hemorrhoids are most common between ages 45 and 65.
Heavy lifting
Repeated heavy lifting (gym, manual labor) increases abdominal pressure.
Obesity
Extra weight increases pressure on pelvic veins.
Genetics
Hemorrhoids tend to run in families. If your parents had them, you’re more likely to develop them.
Abu Dhabi lifestyle factors:
In my Abu Dhabi practice, I see certain patterns: office workers with long sitting hours, dehydration from relying on coffee and tea rather than water, low fiber intake (eating out frequently, processed foods), and delayed medical care because of busy work schedules or embarrassment.
Treatment Options in Abu Dhabi: From Conservative Care to Surgery
Before considering any procedure, we start with lifestyle and dietary changes. For Grade I and early Grade II hemorrhoids, this is often all you need.
Dietary changes: fiber and hydration
- Goal: Softer, bulkier stools that pass easily without straining
- Fiber target: 25–35 grams daily (fruits, vegetables, whole grains, legumes)
- Hydration: Aim for 2.5–3 liters of water daily in Abu Dhabi’s climate (more if you exercise)
- Fiber supplements: Psyllium (Metamucil, Fybogel) or methylcellulose if diet alone isn’t enough
Toilet habits
- Don’t strain or hold your breath
- Don’t sit on the toilet for more than 5 minutes (put your phone away)
- Go when you feel the urge — don’t delay
- Consider a footstool to elevate your knees (squatting position opens the anorectal angle)
Topical treatments
- Over-the-counter creams or suppositories (hydrocortisone, witch hazel, lidocaine) provide temporary symptom relief
- They reduce swelling, itching, and discomfort, but they don’t cure hemorrhoids
- Use them for short-term relief (a few days to a week), not long-term
Sitz baths
- Sitting in warm water (not hot) for 10–15 minutes, 2–3 times daily, especially after bowel movements
- Helps soothe irritation and keep the area clean
- When conservative treatment works:
Grade I and some Grade II hemorrhoids often respond well to these changes. Bleeding may stop within a few weeks, and symptoms improve. If conservative treatment doesn’t help after 4–6 weeks, we move to office procedures.
Office Procedures (for Grade I–II, Some Grade III)
These are done in the office or clinic, usually without general anesthesia. You go home the same day and return to normal activities quickly.
Rubber Band Ligation
Rubber band ligation (RBL) is the most common office procedure for Grade I and II internal hemorrhoids. During the procedure, I place a small rubber band around the base of the internal hemorrhoid using a specialized ligator. This cuts off the blood supply, causing the hemorrhoid to wither and fall off within a few days. It is quick, performed without anesthesia, and patients can return to work the next day.
Frequently Asked Questions
1. Is bleeding always caused by hemorrhoids?
No. While hemorrhoids are a common cause of bright red rectal bleeding in adults, other conditions can also cause bleeding — fissures, fistulas, polyps, inflammatory bowel disease, and colorectal cancer. If you’re bleeding, you need an examination to confirm the cause. This is especially important if you’re over 40, have a family history of colon cancer, or have other symptoms like weight loss or change in bowel habits.
2. Do I need a colonoscopy if I have hemorrhoids?
It depends. If you’re under 40, have no red flag symptoms, and examination clearly shows hemorrhoids as the cause of bleeding, you may not need colonoscopy right away. But if you’re 40 or older and haven’t had colon cancer screening, I recommend colonoscopy even if hemorrhoids are present, because both conditions can coexist, and we don’t want to miss an early cancer or polyp. In the UAE, screening typically begins at age 40, which is earlier than in some countries. This reflects local medical guidelines and population risk factors.
3. Can Grade 2 or Grade 3 hemorrhoids go away on their own?
Grade I hemorrhoids can sometimes resolve with conservative treatment (diet, fiber, hydration) alone. Grade II may improve significantly but often require an office procedure like rubber band ligation for lasting relief. Grade III and IV hemorrhoids rarely resolve on their own — they usually need intervention (THD, laser, or surgery) because the structural prolapse doesn’t correct itself with lifestyle changes alone.
4. What’s the best treatment: banding vs laser vs THD vs surgery?
The best treatment depends on your grade:
Grade I–II: Banding, sclerotherapy, or infrared coagulation are first-line
Grade II–III (internal): Laser or THD are good options
Grade IV or large mixed hemorrhoids: Usually require hemorrhoidectomy
Different treatments work for different grades. The safest approach is matching treatment to your specific anatomy.
5. Is laser treatment really painless and scar-free?
Laser treatment is less painful than traditional hemorrhoidectomy, but it’s not painless. You’ll have discomfort for several days, and you’ll need pain medication. “Scar-free” is also misleading — any procedure that treats tissue creates some healing response, though it’s usually not visible or problematic.
Laser is a valuable tool for the right candidate (Grade II–III internal hemorrhoids), but the marketing around “painless laser surgery” often overpromises.
6. What is a thrombosed hemorrhoid and what should I do?
A thrombosed external hemorrhoid is a clot that forms inside an external hemorrhoid, usually suddenly. It causes a painful, firm lump near the anus. The pain is worst in the first 48–72 hours, then gradually improves as the clot dissolves.
If you’re seen within 48–72 hours, I can remove the clot under local anesthesia, which provides immediate relief. After that window, the pain is often improving on its own, and excision may cause more discomfort than waiting for it to resolve.
7. How painful is hemorrhoidectomy recovery?
The first week after hemorrhoidectomy is uncomfortable — most patients experience moderate to severe pain, especially around bowel movements. However, pain is manageable with medication, stool softeners, and sitz baths. By the second week, pain improves significantly. Most patients are back to light activity within 7–14 days and fully recovered within 4–6 weeks.
Modern pain management techniques (local anesthetic injections during surgery, scheduled pain medication, stool softeners) have made recovery much more tolerable than it was years ago.
8. Are hemorrhoids a sign of cancer?
No. Hemorrhoids are not cancer and don’t turn into cancer. However, hemorrhoids and colorectal cancer can cause similar symptoms (bleeding), and they can coexist. This is why proper examination and screening are important — we don’t want to assume bleeding is “just hemorrhoids” and miss an early cancer.
9. Can pregnancy cause hemorrhoids?
Yes. Pregnancy increases pressure on pelvic veins, and hormonal changes relax vein walls, both of which contribute to hemorrhoids. Straining during delivery can also cause or worsen hemorrhoids. Most pregnancy-related hemorrhoids improve after delivery. Conservative treatment is preferred during pregnancy; procedures or surgery (if needed) are usually postponed until after breastfeeding.
10. What foods help with hemorrhoids?
High-fiber foods that promote soft, bulky stools:
Fruits (berries, apples with skin, pears)
Vegetables (broccoli, carrots, leafy greens)
Whole grains (oats, brown rice, whole wheat bread)
Legumes (lentils, chickpeas, beans)
Adequate hydration (2.5–3 liters of water daily in Abu Dhabi’s climate) just as important as fiber.
Avoid excessive processed foods, low-fiber diets, and chronic constipation triggers (too much cheese, red meat, white bread).
11. Can sitting too long worsen hemorrhoids?
Yes. Prolonged sitting — especially on the toilet — increases pressure on anal veins and can worsen hemorrhoids. If you work a desk job, take short breaks to stand and walk every hour. Don’t sit on the toilet for more than 5 minutes (this means no phone scrolling).
12. Can I exercise with hemorrhoids?
Yes, but avoid exercises that increase abdominal pressure significantly (heavy squats, deadlifts) until symptoms improve. Light to moderate exercise (walking, swimming, yoga) is beneficial — it improves circulation and prevents constipation. Listen to your body; if an activity causes pain, stop.
13. When can I return to work after hemorrhoid treatment?
After office procedures (banding): Next day or within 1–2 days
After laser or THD: 3–7 days for desk jobs, 7–14 days for physical work
After hemorrhoidectomy: 7–14 days for desk jobs, 14–21 days for manual labor
14. Will hemorrhoids come back after treatment?
Recurrence depends on the treatment and whether you address underlying causes (constipation, straining, diet):
Conservative treatment: Symptoms may recur if habits don’t change
Rubber band ligation: Variable recurrence over several years
Laser, THD: Some patients may need additional treatment
Hemorrhoidectomy: Lowest recurrence rates
Maintaining good bowel habits (fiber, hydration, not straining) reduces recurrence risk significantly.
15. What happens during anoscopy?
Anoscopy is a brief examination where I insert a small, lighted scope (anoscope) a few centimeters into the anus to visualize internal hemorrhoids. It takes 1–2 minutes. You’ll feel pressure and possibly mild discomfort, but it’s not painful. Anoscopy is essential for accurate diagnosis — I can’t see internal hemorrhoids without it.
16. Do I need to fast before hemorrhoid treatment?
Office procedures (banding, sclerotherapy): No fasting needed
Procedures under sedation or anesthesia (laser, THD, surgery):
Yes, you’ll need to fast (typically 6–8 hours before the procedure). We’ll give you specific instructions.
17. Can I fly with hemorrhoids?
Yes. Flying doesn’t worsen hemorrhoids, though prolonged sitting may cause discomfort. If you’re flying soon after treatment, bring stool softeners and stay well-hydrated (airplane cabins are very dry).
18. Will insurance cover hemorrhoid treatment in Abu Dhabi?
Most insurance plans in the UAE cover medically necessary hemorrhoid treatment, including office procedures and surgery. Coverage for elective or cosmetic procedures (like removing asymptomatic skin tags) varies. We can check with your insurance provider before treatment.
19. Is hemorrhoid treatment confidential?
Yes. All consultations, examinations, and treatments are completely confidential. We understand that hemorrhoids can feel embarrassing, and we prioritize your privacy at every step.
20. How do I choose a good hemorrhoid doctor in Abu Dhabi?
Look for the following:
Colorectal surgery fellowship training (not just general surgery)
Board certification in colorectal surgery
Experience with the full range of treatments (not just one technique)
Willingness to examine you properly (not diagnosing based on symptoms alone)
Honest discussion of options (not pushing the most expensive procedure)
As a colorectal surgeon with fellowship training and European Board Certification, I’m trained specifically in anorectal conditions and perform the full spectrum of hemorrhoid treatments.
References and Medical Sources
This article is based on current medical evidence and clinical practice guidelines:
1. UAE Colorectal Cancer Screening Guidelines – Abu Dhabi Department of Health recommends screening starting at age 40 for average-risk individuals. Abu Dhabi Public Health Center – Colorectal Cancer
2. Cleveland Clinic Abu Dhabi – Colorectal Cancer Screening Guidelines – Local clinical protocols for UAE population. CCAD Screening
3. Thrombosed External Hemorrhoids Treatment – Evidence for 48-72 hour intervention window. Greenspon J, Williams SB, Young HA, Orkin BA. Thrombosed external hemorrhoids: outcome after conservative or surgical management. Dis Colon Rectum. 2004;47(9):1493-8.
4. Transanal Hemorrhoidal Dearterialization (THD) Outcomes – Success rates for Grade II-III hemorrhoids. Ratto C, Giordano P, Donisi L, et al. Transanal haemorrhoidal dearterialisation (THD) for haemorrhoidal disease: a single-centre study on 1000 consecutive cases. Colorectal Dis. 2017;19(8):750-756.
5. American Society of Colon and Rectal Surgeons Clinical Practice Guidelines – Evidence-based hemorrhoid treatment recommendations. Davis BR, Lee-Kong SA, Migaly J, Feingold DL, Steele SR. The American Society of Colon and Rectal Surgeons Clinical Practice Guidelines for the Management of Hemorrhoids. Dis Colon Rectum. 2018;61(3):284-292.
6. Rubber Band Ligation Effectiveness – Long-term outcomes for hemorrhoid banding. Shanmugam V, Thaha MA, Rabindranath KS, Campbell KL, Steele RJ, Loudon MA. Rubber band ligation versus excisional haemorrhoidectomy for haemorrhoids. Cochrane Database Syst Rev. 2005;(3):CD005034.
Medical Review: Written and reviewed by Prof. Dr. Antonio Privitera. consultant colorectal surgeon, fellowship training at the Mayo Clinic and Royal College of Surgeons (UK), and European Board Certification in Colorectal Surgery.
Need expert treatment for hemorrhoids, anal fissure, or anal fistula? Book a consultation with Dr. Antonio Privitera in Abu Dhabi.
Book Your Appointment
WhatsApp / Phone: +971 55 318 8469
About the Author
