
Rubber band ligation (often just called ‘banding’) is the most common office procedure for internal hemorrhoids. For a full overview of the condition before exploring specific treatments, see our guide to hemorrhoid treatment in Abu Dhabi.
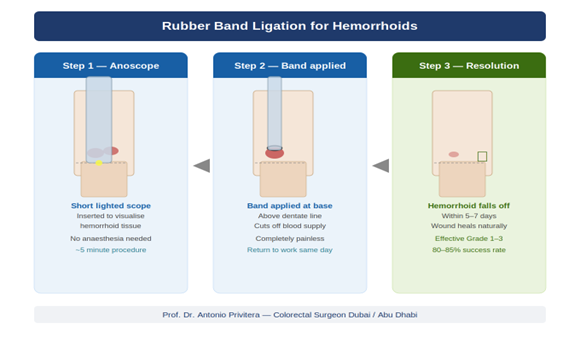
I place a small rubber band around the base of an internal hemorrhoid using a specialized instrument. The band cuts off blood supply. Within 5-10 days, the hemorrhoid withers and falls off (you usually don’t notice when this happens — it passes during a bowel movement).
How It Works
The procedure takes 5-10 minutes and requires no anesthesia. Internal hemorrhoids have no pain receptors, so you feel only mild pressure or a sensation of fullness. I can typically band 1-2 hemorrhoids per session.
If you have multiple hemorrhoids, you may need 2-3 sessions spaced 4-6 weeks apart.
Best For:
- Grade I hemorrhoids (bleed but don’t prolapse)
- Grade II hemorrhoids (prolapse during straining but go back in automatically)
- Small Grade III hemorrhoids (prolapse and require manual reduction)
Not Suitable For:
- Grade III with large external component (banding only treats internal hemorrhoids)
- Grade IV hemorrhoids (permanently prolapsed) Hemorrhoids too close to the dentate line (the band would be painful)
Recovery:
- Day 1: Mild discomfort, feeling of fullness or pressure. Take paracetamol if needed.
- Day 2-7: Most patients feel normal. The banded hemorrhoid is falling off (you usually don’t notice).
- Avoid: Heavy lifting for 3-5 days, straining during bowel movements
Most patients return to work the next day or within 1-2 days.
Success Rate:
Clinical studies show good effectiveness for appropriate grades. The key is patient selection — banding works excellently for Grade I-II but higher recurrence rates for Grade III-IV.
Recurrence: Variable depending on grade and whether lifestyle changes are maintained. Grade I-II patients who maintain high fiber diet and good bowel habits have low recurrence. Grade III patients may experience recurrence and need repeat treatment.
Advantages:
- ✅ Done in office (no operating room, no anesthesia)
- ✅ Minimal downtime (back to work next day)
- ✅ Very low risk
- ✅ Lowest cost
- ✅ Can repeat if needed
Disadvantages:
- ❌ Only treats internal hemorrhoids (not external)
- ❌ Not effective for Grade III-IV
- ❌ May require multiple sessions
- ❌ Moderate recurrence rate for Grade II-III
My Experience:
I perform banding regularly in my Abu Dhabi clinics. When grade is appropriate (I-II), patients are usually very satisfied — minimal discomfort, back to normal quickly, and symptoms resolve. The problems arise when banding is attempted on Grade III-IV hemorrhoids where it’s simply not the right tool for the job.
Laser Hemorrhoidoplasty: The Marketed “Painless” Option
What It Is
Laser hemorrhoid oplasty (LHP) involves inserting a laser fiber into the hemorrhoid tissue and delivering controlled energy. This shrinks the hemorrhoid from the inside by coagulating blood vessels and causing fibrosis (scarring).
How It Works
Done in an operating room under sedation or spinal anesthesia. The procedure takes 20-30 minutes. The laser fiber is inserted into each hemorrhoid through a small puncture, energy is delivered for several seconds per hemorrhoid, and the fiber is withdrawn. No tissue is cut away — the hemorrhoid shrinks over the following weeks.
Best For:
- Grade II internal hemorrhoids (especially if banding has failed or patient prefers single-session treatment)
- Grade III internal hemorrhoids (without significant external component)
Not Suitable For:
- Grade I hemorrhoids (unnecessarily invasive and expensive — banding works just as well)
- Grade IV hemorrhoids (tissue is too prolapsed for laser alone to be effective)
- Large external hemorrhoids (laser targets internal tissue only)
Recovery:
Reality check: Laser is marketed as “painless” and “no downtime,” but this oversells the reality.
- Day 1-3: Moderate discomfort, managed with oral pain medication.
You’ll need stool softeners.
- Day 3-7: Gradual improvement. Most return to desk work by day 5-7.
- Week 2-3: Full recovery, though you’ll need to avoid heavy lifting for 2 weeks.
You will have pain — it’s less than hemorrhoidectomy (traditional surgery), but it’s not “painless.”
Success Rate:
Studies show good short-term results for Grade II-III internal hemorrhoids. Long-term data is more limited compared to banding or THD, as laser for hemorrhoids is newer.
Recurrence: Moderate. Some patients experience symptom recurrence after 1-3 years, though less commonly than with banding.
Advantages:
- ✅ Single session (no repeat appointments)
- ✅ Less pain than traditional hemorrhoidectomy
- ✅ Good for Grade II-III internal hemorrhoids
- ✅ Faster recovery than hemorrhoidectomy
Disadvantages:
- ❌ Overhyped marketing creates unrealistic expectations (“painless,” “no downtime”)
- ❌ Expensive (AED 15,000-25,000 in Abu Dhabi)
- ❌ Doesn’t treat external component
- ❌ Not effective for Grade IV
- ❌ Moderate recurrence rates
- ❌ Less long-term data than older procedures
My Honest Assessment:
Laser is a legitimate option for Grade II-III internal hemorrhoids, especially if you want a single-session treatment and banding has failed or isn’t suitable. However, be skeptical of clinics that push laser for everyone regardless of grade.
Red flags:
- Clinic recommends laser for Grade I hemorrhoids (banding is simpler and equally effective)
- Clinic claims laser is “completely painless” (it’s not)
- Clinic only offers laser and doesn’t perform banding or THD (suggests financial motivation, not clinical judgment)
Laser is a tool, not a miracle. It works well for the right patient but is often oversold.
THD Procedure in Abu Dhabi: Complete Guide to Transanal Hemorrhoidal Dearterialization: The Most Comprehensive Option
What It Is THD
THD, also called HAL-RAR (Hemorrhoidal Artery Ligation with Recto-Anal Repair), is a minimally invasive surgical procedure that addresses hemorrhoids by:
1. Dearterialization: Using Doppler ultrasound, I identify and ligate (tie off) the arteries feeding blood to the hemorrhoids
2. Mucopexy (RAR): I lift and stitch the prolapsed hemorrhoidal tissue back into its normal anatomical position
How It Works
Done in an operating room under spinal or general anesthesia. Takes 45-60 minutes. A specialized proctoscope with Doppler probe is inserted. I identify 4-6 hemorrhoidal arteries and ligate them with absorbable sutures. Then I perform mucopexy — lifting the prolapsed tissue and stitching it back to the rectal wall. No hemorrhoidal tissue is excised (cut away).
Best For:
- Grade II-III internal hemorrhoids (excellent results)
- Select Grade IV (without large external component)
- Patients who’ve failed banding or laser
- Patients who want low recurrence risk
Not Suitable For:
- Grade IV with large external component (external tissue won’t be addressed — hemorrhoidectomy is better)
- Large skin tags (THD doesn’t remove these)
Recovery:
THD is less painful than hemorrhoidectomy because no tissue is cut away.
However, it’s more invasive than laser.
- Day 1-5: Moderate discomfort, managed with oral pain medication and stool softeners. Most patients rest at home.
- Day 5-10: Gradual improvement. Most return to desk work around day 7-10.
- Week 2-4: Full recovery. Avoid heavy lifting for 2-3 weeks.
Success Rate:
Clinical studies show good long-term outcomes for Grade II-III hemorrhoids. One large study of 1,000 patients showed high patient satisfaction with low recurrence at 2-3 years.
Recurrence: Low compared to other minimally invasive procedures. THD addresses both blood supply and anatomical prolapse, which is why it has better durability.
Reference: Ratto C, Giordano P, Donisi L, et al. Transanal haemorrhoidal dearterialisation (THD) for haemorrhoidal disease: a single-centre study on 1000 consecutive cases. Colorectal Dis. 2017;19(8):750-756. PubMed
Advantages:
- ✅ Addresses both blood supply and prolapse (more comprehensive)
- ✅ Low recurrence rates
- ✅ Suitable for Grade III (where banding often fails)
- ✅ Less pain than hemorrhoidectomy
- ✅ Preserves hemorrhoidal tissue (maintains continence)
Disadvantages:
- ❌ Expensive (AED 18,000-30,000 in Abu Dhabi)
- ❌ Requires operating room and anesthesia
- ❌ Longer recovery than banding (5-10 days off work)
- ❌ Doesn’t treat large external components
- ❌ Requires specialized equipment and training (not all surgeons perform it)
My Experience:
THD is my preferred option for Grade III internal hemorrhoids and for Grade II patients who want definitive, low-recurrence treatment. The Doppler technology ensures I’m ligating the correct arteries, and the mucopexy restores anatomy — this combination gives excellent long-term results. However, THD isn’t necessary for Grade I-II that respond to banding, and it won’t fix Grade IV with large external components (those need hemorrhoidectomy).
2. THD Long-Term Outcomes – Large study showing effectiveness. Ratto C, Giordano P, Donisi L, et al. Transanal haemorrhoidal dearterialisation (THD) for haemorrhoidal disease: a single-centre study on 1000 consecutive cases. Colorectal Dis. 2017;19(8):750-756. PubMed
3. American Society of Colon and Rectal Surgeons Guidelines – Evidence-based treatment recommendations. Davis BR, Lee-Kong SA, Migaly J, Feingold DL, Steele SR. The American Society of Colon and Rectal Surgeons Clinical Practice Guidelines for the Management of Hemorrhoids. Dis Colon Rectum. 2018;61(3):284-292. PubMed
4. Laser Hemorrhoidoplasty Review – Current evidence and outcomes. Maloku H, Gashi Z, Lazovic R, Islami H, Juniku-Shkololli A. Laser Hemorrhoidoplasty Procedure vs Open Surgical Hemorrhoidectomy: a Trial Comparing 2 Treatments. JAMA Surg. 2015;150(10):931-936. PubMed
Medical Review: Written and reviewed by Prof. Dr. Antonio Privitera, consultant colorectal surgeon, fellowship training at the Mayo Clinic and Royal College of Surgeons (UK), and European Board Certification in Colorectal Surgery.
Need expert treatment for hemorrhoids, anal fissure, or anal fistula? Book a consultation with Dr. Antonio Privitera in Abu Dhabi.
Book Your Appointment
WhatsApp / Phone: +971 55 318 8469
About the Author
