
Fistulotomy – laying open the fistula tract – is the most effective and most commonly performed operation for simple anal fistulas. When the anatomy is appropriate (simple, low fistula with minimal sphincter involvement), fistulotomy achieves cure rates exceeding 90%, with rapid recovery and low recurrence. For a complete overview of all fistula treatment options, see our anal fistula treatment in Dubai.
The challenge is patient selection: fistulotomy is safe for simple fistulas and potentially harmful for complex ones. This guide explains what the operation involves, who it is suitable for, and what to expect.
What Is Fistulotomy?
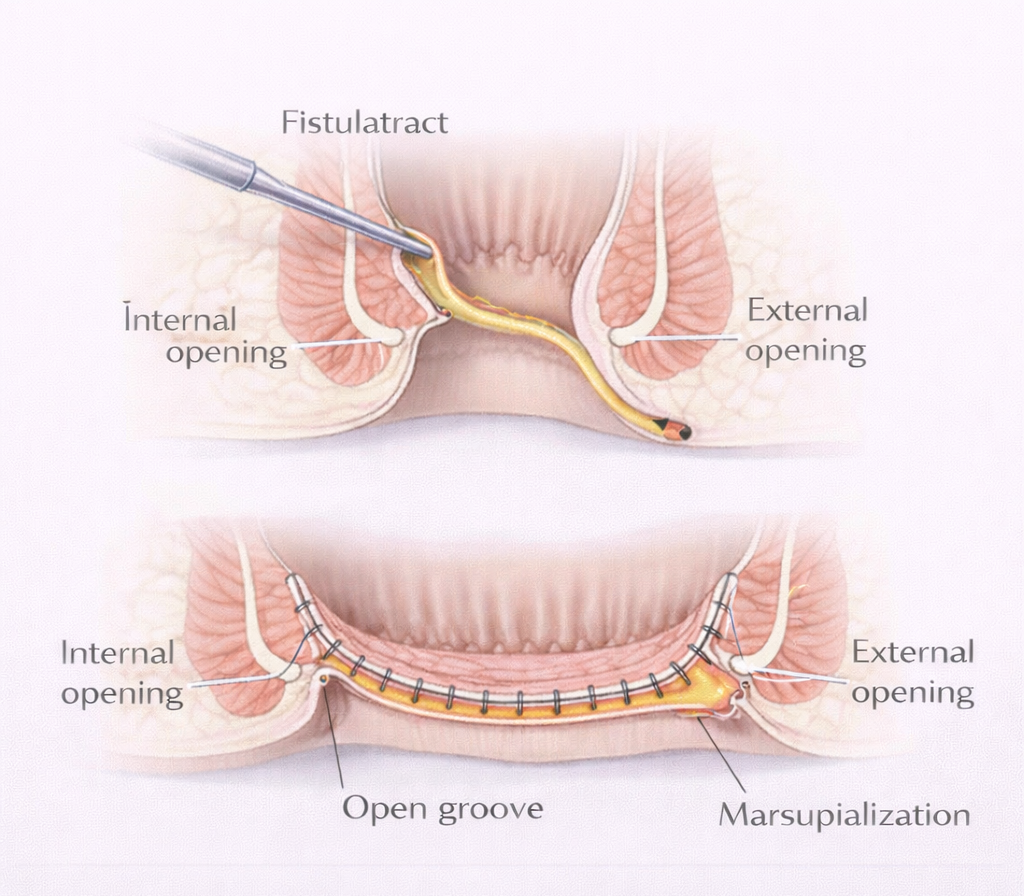
Fistulotomy means ‘opening of the fistula’. The surgeon:
- Identifies the fistula tract from the external opening to the internal opening in the anal canal
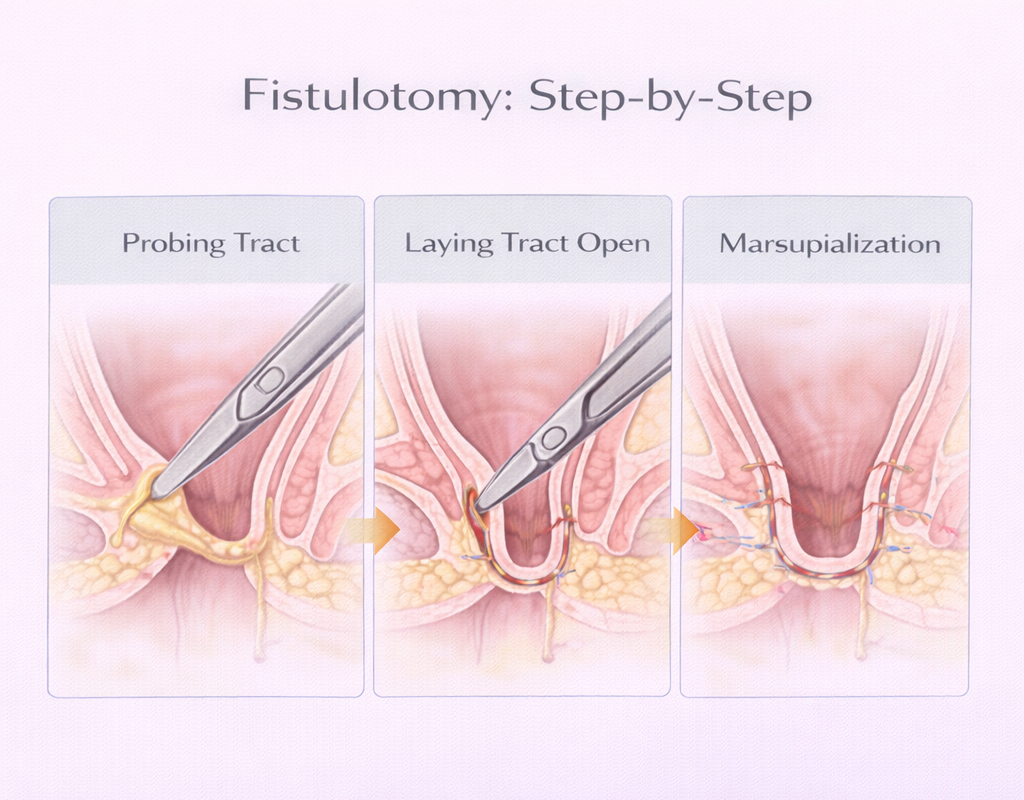
- Probes the tract carefully to map its course in relation to the sphincters
- Lays the tract open cuts along it so it becomes a groove rather than a tunnel
- Marsupializes the edges stitches the edges of the groove to the surrounding skin to keep it open and allow healing from the base
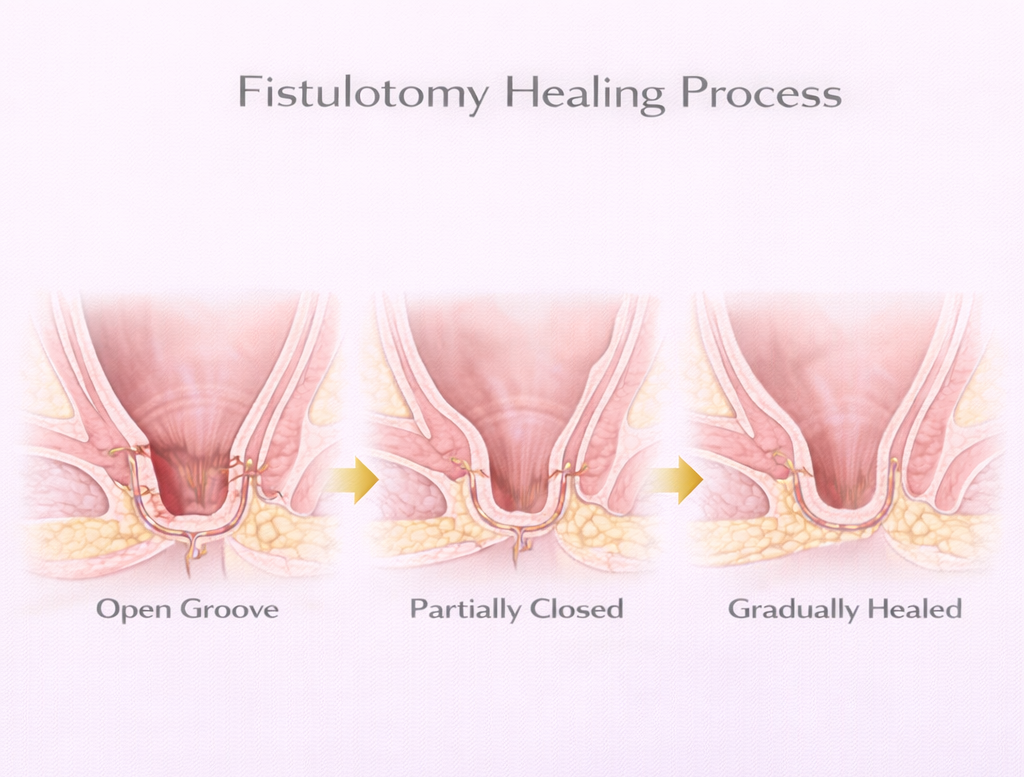
The wound heals by secondary intention (from the base upward) over 4-8 weeks.
Who Is Suitable for Fistulotomy?
Suitable
- Intersphincteric fistulas: The entire internal sphincter from the internal opening to the external opening can be divided the external sphincter is not involved, so continence is unaffected
- Low transsphincteric fistulas: Involving only the lower 1/3 of the external sphincter in a patient with good preoperative sphincter function
NOT Suitable
- High transsphincteric fistulas: Dividing the upper 2/3 of the external sphincter causes significant incontinence
- Suprasphincteric or extrasphincteric fistulas
- Female patients with anterior fistulas (near the midline in women with short anterior perineum high incontinence risk)
- Patients with pre-existing sphincter weakness or incontinence
- Crohn’s fistulas – wound healing is poor, and fistulotomy typically fails
Fistulotomy is safe for simple fistulas but not for complex ones involving significant sphincter muscle. Complex cases differ. See complex fistula treatment.
The Procedure: What to Expect
Before Surgery
- Day-case procedure – home same day in most cases
- General or spinal anesthesia
- No bowel preparation required
- Fast for 4-6 hours before surgery
During Surgery
- Examination under anesthesia (EUA): The fistula is probed to confirm the internal opening and map the tract
- If the anatomy is as expected (simple fistula) → fistulotomy proceeds
- If the anatomy is more complex than anticipated → a seton may be placed instead (the surgeon will not perform a fistulotomy on an unexpectedly complex fistula)
- Duration: 30-60 minutes
After Surgery
- Mild to moderate wound pain for 1-2 weeks
- Wound care: Keep the wound clean sitz baths or showering after bowel movements. Wound dressings as instructed.
- Stool softeners: Essential passing a soft stool is important for wound healing and comfort
Recovery
- Work (desk): 5-10 days
- Work (manual): 2-4 weeks
- Exercise: Light walking from day 1. Gym: 4 weeks.
- Full wound healing: 4-8 weeks (the wound heals from the base it takes time but is reliable)
Results
- Cure rate: >90% for simple intersphincteric and low transsphincteric fistulas
- Recurrence: <10% – usually indicates an unidentified secondary tract or residual internal opening. See recurrence risk.
- Incontinence: Very low for appropriate patients minor transient
incontinence to gas is possible; significant fecal incontinence is rare with correct patient selection
Need expert treatment for hemorrhoids, anal fissure, or anal fistula? Book a consultation with Dr. Antonio Privitera in Dubai or Abu Dhabi.
📱 WhatsApp: +971 55 318 8469
📞 Phone: +971 55 318 8469
References
- Steele SR et al. Practice parameters for the management of perianal abscess and fistula-in-ano. Dis Colon Rectum. 2011.
Need expert treatment for hemorrhoids, anal fissure, or anal fistula? Book a consultation with Dr. Antonio Privitera in Dubai or Abu Dhabi.
📱 WhatsApp: +971 55 318 8469
📞 Phone: +971 55 318 8469
AUTHOR AUTHORITY BLOCK
Fellowship-trained at Mayo Clinic (USA) and the Royal College of Surgeons (UK). Member of the Royal College of Surgeons of Edinburgh. Certified in General Surgery by the Italian Medical Council.
About the Author
