
Lateral internal sphincterotomy (LIS) is the most effective surgical treatment for chronic anal fissure. For a complete overview of all treatment options, see anal fissure treatment in Dubai.
I perform LIS regularly in Dubai and Abu Dhabi. This guide explains exactly what the procedure involves, what to expect, and how to decide if it is the right treatment for your situation.
- Indication: chronic fissure not responding to medical treatment
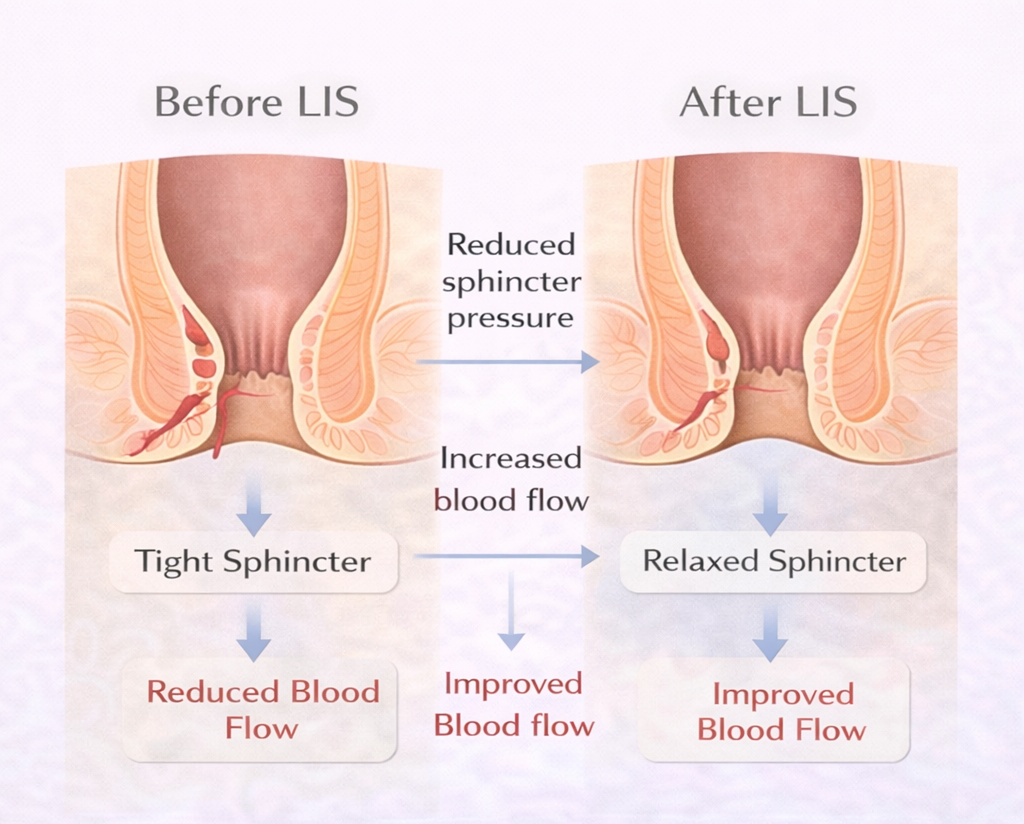
- Goal: reduce sphincter pressure and allow healing
- Outcome: high healing rate with low recurrence
What Is Lateral Internal Sphincterotomy?
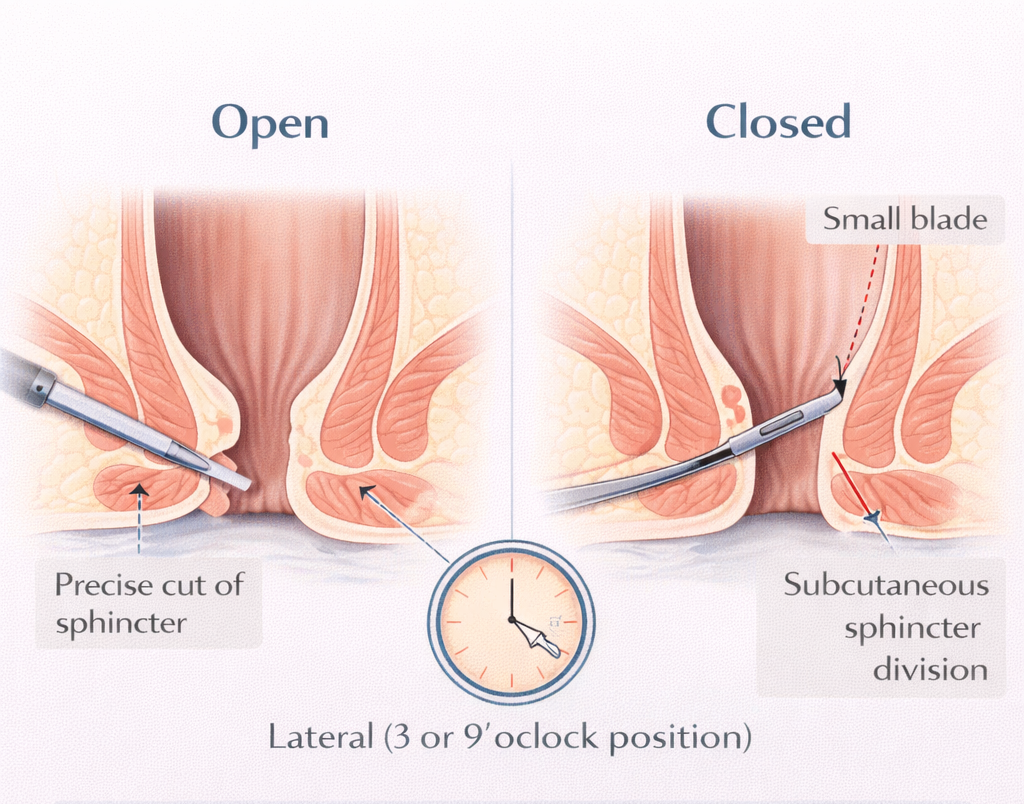
LIS involves dividing part of the internal anal sphincter the involuntary muscle whose spasm causes chronic fissures and prevents healing. By making a precise cut in this muscle, we permanently reduce resting anal pressure, restore blood supply to the posterior midline, and allow the fissure to heal.
The word ‘lateral’ is important: the cut is made at the 3 or 9 o’clock position (the side), NOT at the site of the fissure (the back). This is deliberate cutting at the fissure site (‘posterior sphincterotomy’) carries higher incontinence risk and has been largely abandoned. Understanding chronic fissures is essential. See why chronic fissures don’t heal.
The Procedure: Step by Step
Before Surgery
- Day-case procedure you arrive in the morning and go home the same day
- General anesthesia (most common), spinal anesthesia, or local anesthesia with sedation
- No bowel preparation required
- Fast for 4-6 hours before surgery (solids)
During Surgery
- You are positioned in lithotomy (on your back, legs raised) or prone (face down)
- The procedure takes 15-30 minutes
- Two techniques: Open (a small skin incision is made and the sphincter is divided under direct vision) or Closed/subcutaneous (a fine blade is passed into the intersphincteric groove and the sphincter divided without a skin incision most common in UAE)
- The sentinel pile (if present) and any hypertrophied papilla may be excised at the same time
After Surgery
- Recover in the day-surgery unit for 1-3 hours
- Go home when pain is controlled and you have passed urine
- Some patients experience temporary difficulty with urination immediately after surgery this is normal and resolves
Recovery
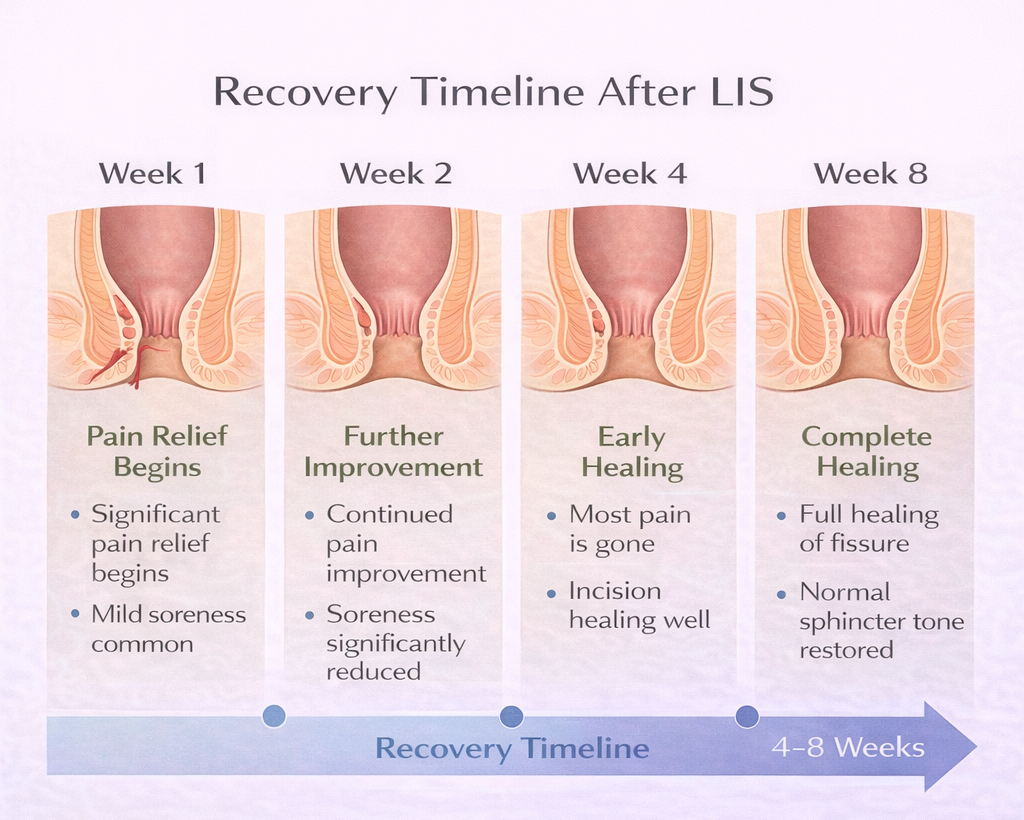
- Pain: Significant improvement is usually noticed within 1-2 weeks as the spasm is relieved. The wound itself may be tender for 2-4 weeks.
- Work: Desk work: 3-7 days.
- Manual labor: 2-4 weeks.
- Driving: 3-7 days (until you are off narcotic pain relief and comfortable)
- Exercise: Light walking from day 1.
- Gym and heavy lifting: 4 weeks.
- Full healing: 4-8 weeks
Results
- Healing rate: >95% for appropriately selected chronic fissures
- Pain relief: Most patients experience significant or complete relief within 2 weeks of surgery
- Recurrence: Very low <5% in most series
Risks and Side Effects
Incontinence – The Most Important Risk
The most significant risk of LIS is minor fecal incontinence difficulty controlling gas or liquid stool. The reported rate varies widely (1-30% depending on how it is measured and how long patients are followed), but significant, persistent incontinence with solid stool is rare in experienced hands.
Risk factors for incontinence after LIS: prior anorectal surgery, sphincter injury from childbirth, low preoperative sphincter pressure. These are assessed before deciding to proceed with surgery.
Other Risks
- Infection: Uncommon the perianal area has good blood supply
- Bleeding: Minor, usually self-limiting
- Fissure recurrence: <5%
- Incomplete healing: Rare usually indicates Crohn’s disease or other underlying condition
LIS vs Botox: Which Is Right for You?
I discuss this with every patient individually. In general:
- LIS is preferred when: Creams and Botox have failed; the patient has very high resting sphincter pressure; the fissure has been chronic for years; the patient wants a definitive, one-time treatment and understands the incontinence risk.
- Botox is preferred when: The patient wants to avoid surgery; the fissure is moderately chronic; the patient is concerned about incontinence risk; first-line treatment failure.
This is usually considered after conservative treatment fails. Learn more about Botox treatment for fissure.
References
- American Society of Colon and Rectal Surgeons. Practice parameters for the management of anal fissures. Dis Colon Rectum. 2017.
- Altomare DF et al. Lateral internal sphincterotomy for chronic anal fissure. Br J Surg. 2019.
Need expert treatment for hemorrhoids, anal fissure, or anal fistula? Book a consultation with Dr. Antonio Privitera in Dubai or Abu Dhabi.
📱 WhatsApp: +971 55 318 8469
📞 Phone: +971 55 318 8469
AUTHOR AUTHORITY BLOCK
Fellowship-trained at Mayo Clinic (USA) and the Royal College of Surgeons (UK). Member of the Royal College of Surgeons of Edinburgh. Certified in General Surgery by the Italian Medical Council.
About the Author
