
Hemorrhoids during pregnancy in Dubai are common because of increased pelvic pressure, hormonal changes, and constipation. Most cases can be managed safely with conservative treatment and specialist advice. For a full treatment overview including options safe during pregnancy, see our hemorrhoid treatment in Dubai. might develop them. You’ve heard they’re common during pregnancy, but you’re not sure what’s safe to do about them. Can you take medication?
Do you need to see a doctor? Will they go away after delivery?
I’m Professor Dr. Antonio Privitera, a consultant colorectal surgeon with fellowship training at the Mayo Clinic and Royal College of Surgeons (UK), practicing across Dubai. I work with expectant mothers regularly, often in coordination with their obstetricians, to manage hemorrhoids safely during pregnancy and postpartum.
Here’s what you need to know:
- Hemorrhoids affect up to 50% of pregnant women (you’re not alone)
- They’re caused by pregnancy-specific factors: increased pressure, hormones, constipation
- Most treatments are postponed until after breastfeeding, but saf symptom management exists
- Most pregnancy hemorrhoids improve significantly within 2-3 months postpartum
- Some women need treatment postpartum if symptoms persist
This comprehensive guide covers:
- Why pregnancy causes hemorrhoids
- Prevention strategies for each trimester
- Safe treatments during pregnancy
- Managing hemorrhoids during labor and delivery
- Postpartum hemorrhoid care
- When to see a specialist
For safe hemorrhoid management during or after pregnancy:
Experiencing symptoms like these? A discreet same-day specialist assessment is available across Dubai .
WhatsApp: +971 55 318 8469 | Phone: +971 55 318 8469
Medcare Discovery Gardens (Dubai)

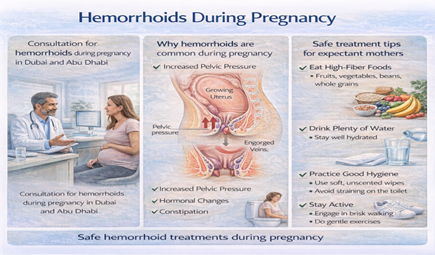
Why Pregnancy Causes Hemorrhoids
Four Main Causes:
1. Increased Pelvic Pressure
- Growing uterus puts direct pressure on pelvic veins
- Pressure increases as baby grows (worst in third trimester)
- Blood pools in hemorrhoidal veins
- Veins stretch and swell
2. Hormonal Changes
- Progesterone levels increase dramatically during pregnancy
- Progesterone relaxes vein walls (makes them stretch more easily)
- Also relaxes intestinal muscles (contributes to constipation)
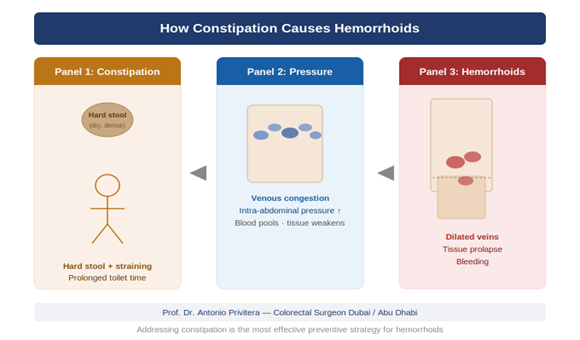
3. Constipation
- Hormonal changes slow intestinal transit
- Prenatal vitamins (especially iron) can worsen constipation
- Straining during bowel movements increases hemorrhoid risk
- This can start as early as first trimester
4. Increased Blood Volume
- Blood volume increases 40-50% during pregnancy
- More blood flow through all veins, including hemorrhoidal veins
- Contributes to vein engorgement
Risk Peaks:
Third Trimester:
- Maximum uterus size = maximum pelvic pressure
- Accumulated months of constipation
- Baby’s head putting pressure on pelvic veins
- Many women develop hemorrhoids weeks 32-40
Labor and Delivery:
- Pushing during labor creates enormous pressure
- Can cause new hemorrhoids or worsen existing ones
- Very common to develop hemorrhoids during delivery
Postpartum:
- Some hemorrhoids appear or worsen in first 2 weeks after delivery
- Related to delivery strain + early postpartum constipation
Prevention Strategies: Starting in First Trimester
First Trimester (Weeks 1-12):
Start prevention NOW—before problems develop:
Diet:
- High-fiber foods from the start
- Fruits, vegetables, whole grains, legumes
- Target 25-35g fiber daily
- Combat early pregnancy nausea with small, frequent fiber-rich meals
Hydration:
- 2.5-3 liters water daily (more in Dubai heat)
- Helps soften stools
- Counteracts dehydrating effect of progesterone
Prenatal Vitamins:
- Take with food to minimize constipation
- If iron in prenatal causes severe constipation, discuss with OB
about alternatives (iron-free prenatal + separate iron supplement that’s better tolerated)
Bowel Habits:
- Don’t delay when you feel urge
- Don’t strain
- Maximum 5 minutes on toilet
Second Trimester (Weeks 13-26):
Constipation often worsens—stay vigilant:
Continue fiber and hydration (as above)
Add:
- Fiber supplement if diet alone isn’t enough (psyllium is safe during pregnancy)
- Safe stool softeners if constipated: docusate (Colace), lactulose—discuss with OB
- Gentle exercise: Walking 20-30 minutes daily (improves bowel motility, safe throughout pregnancy)
Positioning:
- As belly grows, sleeping on left side improves circulation and reduces pressure on rectal veins
Third Trimester (Weeks 27-40):
Highest risk period—maximize prevention:
Continue all above, plus:
Avoid prolonged standing or sitting:
- Take breaks every hour to walk/change position
- Use pregnancy pillow for comfortable side-lying
Pelvic floor exercises (Kegels):
- Strengthen pelvic floor (helps with delivery too)
- May reduce hemorrhoid risk by improving circulation
Don’t gain excessive weight:
- Follow OB’s weight gain recommendations
- Excess weight increases pelvic pressure
Prepare for postpartum:
- Stock up: stool softeners, fiber supplements, sitz bath basin, topical hemorrhoid cream
- You’ll want these ready after delivery
Safe Treatments During Pregnancy
What You CAN Do:
Conservative Management (Safe Throughout Pregnancy):
1. Dietary Fiber:
- Completely safe
- Most important intervention
- Prevents constipation = prevents straining
2. Increased Water Intake:
- Safe and necessary
3. Stool Softeners:
- Docusate (Colace): Safe during pregnancy
- Lactulose: Safe during pregnancy
- Polyethylene glycol (Miralax): Generally considered safe, discuss with OB
4. Topical Treatments:
- Witch hazel pads: Safe (Tucks pads, preparation H wipes)
- Hydrocortisone cream (1%): Safe for short-term use (few days at a time)
- Lidocaine gel: Safe for temporary pain relief
- Preparation H ointment: Safe (external use)
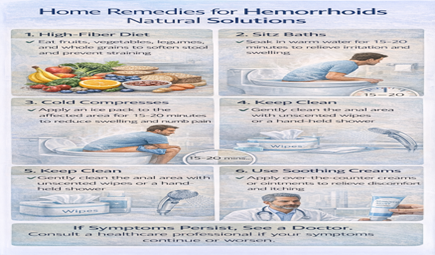
5. Sitz Baths:
- Completely safe and very helpful
- Warm (not hot) water, 10-15 minutes, 2-3 times daily
- Reduces pain and inflammation
6. Ice Packs:
- Safe for acute swelling or thrombosed hemorrhoid
- 10-15 minutes, wrapped in cloth
7. Positioning:
- Lie on left side (reduces pressure on rectal veins)
- Use pillows to elevate hips slightly when resting
What to AVOID During Pregnancy:
Medications:
- Oral pain medications: Paracetamol is safe; NSAIDs (ibuprofen) are NOT safe in third trimester
- Laxatives: Avoid stimulant laxatives (senna, bisacodyl) unless OB approves—can cause uterine contractions
Procedures:
- Rubber band ligation: Postponed until after pregnancy/breastfeeding
- Laser, THD, surgery: Postponed until after pregnancy/breastfeeding
- Thrombosed hemorrhoid excision: Can be done if absolutely necessary, but usually managed conservatively during pregnancy
Why procedures are postponed:
- Anesthesia risks to baby
- Positioning difficulties (lying on procedure table while pregnant)
- High chance hemorrhoids will improve postpartum anyway
- Recovery is harder during pregnancy
If symptoms persist or are not improving, a specialist assessment in Dubai can help determine the most appropriate treatment.
Managing Hemorrhoids During Labor and Delivery
Before Labor:
Discuss with your OB:
- Mention if you have hemorrhoids
- They can note this and potentially make delivery adjustments
Stool management:
- Some women have bowel movement at start of labor (normal)
- Don’t be embarrassed—OBs and nurses deal with this constantly
During Delivery:
Pushing phase:
- This is when hemorrhoid risk is highest
- Your OB will guide you on pushing technique
- They’ll support perineum which helps reduce hemorrhoid prolapse
If hemorrhoids prolapse during pushing:
- Very common
- Usually reduce (go back in) after delivery
- Midwives/nurses will check after delivery
Immediately Postpartum:
First 24 Hours:
- You may notice hemorrhoids are worse than before delivery
- Swelling, pain, prolapse are common
- Thrombosed hemorrhoid (clot) can develop
Management:
- Ice packs first 24-48 hours
- Sitz baths after that
- Topical treatments (witch hazel, hydrocortisone)
- Stool softeners (you’ll receive these in hospital)
- Pain medication as prescribed
First bowel movement:
- Usually 1-3 days postpartum
- You’ll be afraid to go (between delivery soreness and hemorrhoids)
- Take stool softeners as prescribed
- Don’t strain
- It will be uncomfortable but manageable
Postpartum Hemorrhoid Management
First 6-8 Weeks:
What to expect:
- Most pregnancy-related hemorrhoids improve significantly
- Swelling decreases as pregnancy-related pressure resolves
- Some hemorrhoids resolve completely
- Others shrink but remain
Management:
Continue:
- High-fiber diet (especially important if breastfeeding—needs more calories, more fiber)
- Hydration (essential for breastfeeding)
- Stool softeners as needed
- Sitz baths
- Topical treatments
Breastfeeding considerations:
- Most topical hemorrhoid treatments are safe while breastfeeding
- Oral pain medication: Paracetamol safe, ibuprofen safe, avoid codeine/opioids if possible
- Discuss any medications with pediatrician if concerned
Rest and recovery:
- You’re recovering from delivery + managing newborn care
- Don’t rush hemorrhoid treatment if symptoms are manageable
After 6-8 Weeks:
6-week postpartum checkup:
- Discuss hemorrhoids with your OB
- If symptoms are improving, continue conservative management
- If symptoms persist or worsen, consider referral to colorectal surgeon
When to seek treatment:
- Bleeding continues beyond 8 weeks postpartum
- Pain interferes with caring for baby
- Hemorrhoids are prolapsed (won’t stay inside)
- Quality of life significantly impacted
Treatment options postpartum:
- Once breastfeeding is finished (or OB clears you), full range of
treatments available
- Rubber band ligation for Grade I-II
- Laser or THD for Grade III
- Hemorrhoidectomy for Grade IV or if other treatments failed
Many women wait 6-12 months postpartum before pursuing treatment:
- Focused on baby during first months
- Giving hemorrhoids time to naturally improve
- Waiting until breastfeeding finished
- This is perfectly reasonable if symptoms are manageable
When to See a Doctor During Pregnancy
Call Your OB If:
Urgent:
- Heavy bleeding from rectum (soaking through pad)
- Severe pain not relieved by conservative measures
- Fever with anal pain (possible infection/abscess)
- Inability to reduce prolapsed hemorrhoid (strangulation concern)
Non-Urgent (Mention at Next Appointment):
- Persistent bleeding (small amounts)
- Discomfort interfering with daily activities
- Concerns about hemorrhoids and delivery
- Questions about safe treatments
When to See Colorectal Surgeon:
During pregnancy (rare):
- Thrombosed hemorrhoid within 48-72 hour window (can be excised under local anesthesia if severe pain)
- Complicated hemorrhoids not responding to conservative care
- Diagnostic uncertainty (is it hemorrhoids or something else?)
Postpartum:
- If symptoms persist beyond 8 weeks and interfering with life
- If you want definitive treatment after breastfeeding
- For proper grading and treatment recommendation
Special Considerations for Dubai/UAE
Climate Factors:
Dehydration risk:
- Dubai heat, even with AC
- Increased fluid needs during pregnancy
- Breastfeeding increases needs even more
- Target 3+ liters daily
Lifestyle:
Expatriate community:
- May have less family support postpartum
- Hemorrhoid management while caring for newborn alone is harder
- Consider hiring postpartum support if available
Healthcare access:
- Excellent maternal healthcare in Dubai
- Easy access to colorectal surgeons if needed
- Insurance usually covers pregnancy-related complications including hemorrhoids
Cultural Considerations:
Privacy concerns:
- Many women hesitant to discuss hemorrhoids
- Know that OBs and colorectal surgeons deal with this constantly during pregnancy
- Your comfort and health are priorities
Modesty:
- Female colorectal surgeons available if preferred
- Chaperones always available during examinations
Preventing Hemorrhoids in Future Pregnancies
If you had hemorrhoids with first pregnancy:
Before conceiving again:
- Optimize bowel health (high fiber, good hydration)
- Treat any existing hemorrhoids if symptomatic
- Achieve healthy weight
During next pregnancy:
- Start prevention strategies from week 1
- Be extra vigilant about fiber and hydration
- Use stool softeners earlier if needed
- Discuss with OB early on
Likelihood of recurrence:
- If you had hemorrhoids with first pregnancy, higher risk with subsequent pregnancies
- But: Good prevention can minimize or prevent recurrence
This article is written and reviewed by Prof. Dr Antonio Privitera, consultant colorectal surgeon with fellowship training at Mayo Clinic (USA) and the Royal College of Surgeons (UK), specializing in hemorrhoid diagnosis and minimally invasive treatment.
Frequently Asked Questions
1. Will hemorrhoids go away after delivery?
Many improve significantly within 6-8 weeks postpartum. Some resolve completely. Others shrink but remain. If symptomatic beyond 8 weeks, treatment options are available.
2. Can I have hemorrhoid surgery while pregnant?
Elective hemorrhoid surgery is postponed until after pregnancy and ideally after breastfeeding. Emergency procedures (thrombosed hemorrhoid excision) can be done if necessary.
3. Are stool softeners safe during pregnancy?
Yes. Docusate (Colace) and lactulose are safe throughout pregnancy. Discuss with your OB
4. Can I use Preparation H while pregnant?
Yes, Preparation H ointment for external use is considered safe during pregnancy. Avoid suppositories without discussing with OB.
5. Will pushing during labor make hemorrhoids worse?
It can. Many women develop new hemorrhoids or worsen existing ones during delivery. This is very common and expected.
6. Should I have a C-section if I have severe hemorrhoids?
No. Hemorrhoids alone are not an indication for C-section. C-section has its own risks and recovery. Vaginal delivery is still the recommendation unless there are other obstetric reasons for C-section.
7. Can I breastfeed if I need hemorrhoid treatment?
Yes. Most topical treatments are safe while breastfeeding. If you need procedures (banding, laser, surgery), discuss timing with your OB and colorectal surgeon.
8. Will hemorrhoids affect my ability to care for my baby?
Mild to moderate hemorrhoids usually don’t interfere significantly. Severe hemorrhoids can cause pain that makes sitting, lifting, or moving difficult. Seek treatment if this is the case.
9. Can I prevent hemorrhoids completely during pregnancy?
Not always. Even with perfect prevention strategies, some women develop hemorrhoids due to pregnancy-related pressure and hormones. But prevention significantly reduces risk and severity.
10. When can I have definitive hemorrhoid treatment postpartum?
Usually after breastfeeding is complete, or at least 6-12 months postpartum. Conservative management is used until then unless symptoms are severe.
References and Medical Sources
Pregnancy hemorrhoid management based on evidence:
1. Hemorrhoids in Pregnancy: Prevalence and Treatment – Clinical review. Poskus T, Buzinskienė D, Drasutiene G, et al. Haemorrhoids and anal fissures during pregnancy and after childbirth: a prospective cohort study. BJOG. 2014;121(13):1666-71. PubMed
2. Safe Medications During Pregnancy – Treatment guidelines. American College of Obstetricians and Gynecologists. ACOG Committee Opinion on Hemorrhoids in Pregnancy.
3. Postpartum Hemorrhoid Management – Recovery timeline. Abramowitz L, Sobhani I, Benifla JL, et al. Anal fissure and thrombosed external hemorrhoids before and after delivery. Dis Colon Rectum. 2002;45(5):650-5. PubMed
Medical Review: This content was written and reviewed by Professor training at the Mayo Clinic and Royal College of Surgeons (UK), and European Board Certification in Colorectal Surgery.
Pregnancy and Postpartum Hemorrhoid Care in Dubai
Safe, gentle treatment options for expectant and new mothers.
Experiencing symptoms like these? A discreet same-day specialist assessment is available across Dubai .
WhatsApp: +971 55 318 8469 | Phone: +971 55 318 8469
Medcare Discovery Gardens (Dubai)
Dubai Locations
- Medcare Women and Children Hospital (Specialized maternity care)
- Medcare Royal Specialty Hospital
- Other locations available
We coordinate with your OB/GYN for comprehensive care.
Professor Dr. Antonio Privitera
Fellowship Training: Mayo Clinic | Royal College of Surgeons (UK)
European Board Certified in Colorectal Surgery ✅ DAY 14: BEST FOODS FOR HEMORRHOIDS DUBAI
About the Author
