
Hemorrhoidectomy recovery in Dubai depends on the procedure performed and the individual patient, but most people improve progressively over the first few weeks. Knowing what to expect makes recovery safer and less stressful, see our hemorrhoid treatment in Dubai. scheduled for it soon and want to know exactly what to expect. You’ve heard hemorrhoid surgery recovery is painful, and you’re anxious about the first bowel movement. You’re wondering when you can return to work, when you can exercise again, and how long until you feel normal.
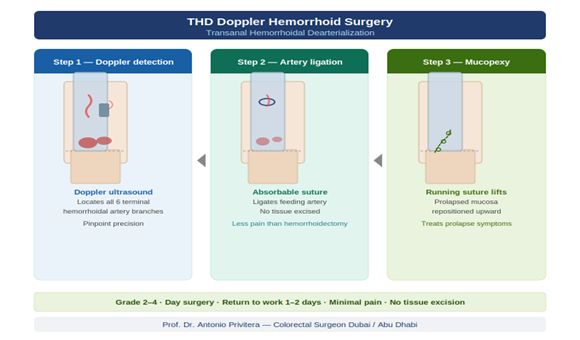
Let me give you the honest, detailed timeline—no sugarcoating, but also no unnecessary fear. I’m Professor Dr. Antonio Privitera, a consultant colorectal surgeon with fellowship training at the Mayo Clinic and Royal College of Surgeons (UK), practicing across Dubai. I perform hemorrhoidectomy regularly, and I guide patients through recovery every week.
The bottom line upfront: Hemorrhoidectomy recovery IS uncomfortable, especially the first week. But with proper pain management, realistic expectations, and the right strategies, it’s manageable. Most patients tell me afterward: “It was tough but not as bad as I feared, and I’m so glad I did it.”
This comprehensive guide covers:
- Day-by-day recovery timeline (what to expect each day)
- Pain management strategies that actually work
- The first bowel movement (and how to make it less scary)
- When to return to work, exercise, sex, travel
- Warning signs of complications
- Tips from patients who’ve been through it
For post-operative support or pre-operative consultation:
Experiencing symptoms like these? A discreet same-day specialist assessment is available across Dubai.
WhatsApp: +971 55 318 8469 | Phone: +971 55 318 8469
Medcare Discovery Gardens (Dubai)
Before We Start: Setting Realistic Expectations
Three Things to Know:
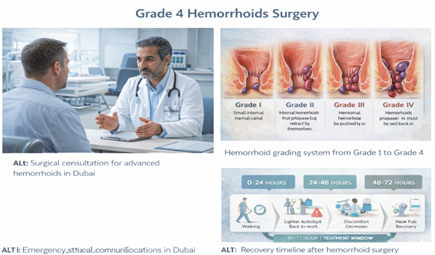
1. The First Week Is the Hardest
- Pain peaks days 1-3, then gradually improves
- First bowel movement (day 2-3) is anxiety-inducing but manageable
- You’ll need strong pain medication and stool softeners
2. Recovery Is Gradual, Not Linear
- Some days feel better, some feel worse (this is normal)
- Each week is noticeably better than the previous week
- Full healing takes 6-8 weeks, but you’ll feel much better by week
3. Pain Management Is Key
- Take pain medication ON SCHEDULE (don’t wait until pain is severe)
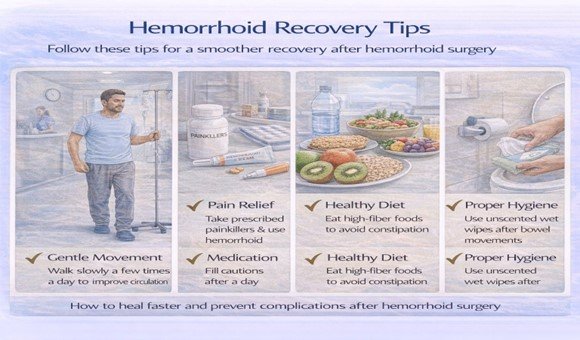
- Stool softeners are NON-NEGOTIABLE (start immediately, continue for 2-4 weeks)
- Sitz baths 3-4 times daily make a huge difference
Now let’s walk through recovery week by week.
Week 1: The Hardest Week (Days 1-7)
Day 1 (Surgery Day):
At the hospital:
- You wake up in recovery room
- Pain medication is on board (you may feel groggy but comfortable initially)
- Once you’re stable and able to urinate, you’re discharged (usually 2-4 hours post-surgery)
- You’ll receive prescriptions: pain medication, stool softeners, possibly antibiotics
At home:
- Pain level: 4-6/10 (anesthesia and initial pain meds still working)
- What to do: Rest, ice packs to area (wrapped in cloth, 15 minutes on/off), start sitz baths in evening
- Medications: Take pain medication as prescribed (don’t skip doses), start stool softener immediately
- Food: Light, soft foods (avoid spicy or difficult-to-digest foods)
- You haven’t had a bowel movement yet (this is normal and expected)
Sleep: Difficult to get comfortable. Try:
- Sleeping on your side with pillow between knees
- Lying on stomach with pillow under hips
- Avoid sleeping flat on back (increases pressure on surgical area)
Days 2-3: Peak Pain Phase
The First Bowel Movement (Usually Day 2-3):
This is what patients fear most. Let’s address it directly:
Your anxiety is normal. Every patient worries about this.
Here’s what actually happens:
- You’ll feel the urge (don’t delay—go when you feel it)
- Sit on toilet (bring your stool softener bottle, pain medication, and patience)
- Take slow, deep breaths (don’t hold breath or strain)
- The stool should be soft because you’ve been taking stool softeners
- Yes, it will sting/burn. Pain level: 7-9/10 for the few minutes you’re passing stool
- But: It’s brief (2-5 minutes of active discomfort), and each subsequent bowel movement is easier
Immediately after first bowel movement:
- Take sitz bath (warm water, 15 minutes)
- Apply topical anesthetic if prescribed
- Take pain medication if needed
- Lie down and rest
Critical mistakes to avoid:
- ❌ Delaying bowel movement out of fear (makes stool harder and more painful)
- ❌ Straining or pushing (absolutely don’t strain)
- ❌ Skipping stool softeners (“I don’t feel constipated”) → Take them anyway
Pain level (Days 2-3): 7-9/10 during bowel movements, 5-7/10 at rest
Medications:
- Pain medication every 4-6 hours (don’t wait until pain is unbearable)
- Stool softener 2-3 times daily
- Continue for full duration prescribed
Activities:
- Rest at home
- Short walks around house encouraged (promotes circulation, prevents blood clots)
- Sitz baths 3-4 times daily (after each bowel movement + before bed minimum)
- No prolonged sitting (lie down or walk, avoid sitting >15 minutes at a time)
Food:
- Soft, easily digestible foods
- High fluid intake (2-3 liters daily)
- Avoid: spicy foods, alcohol, caffeine (can irritate bowels)
Days 4-7: Early Improvement
Pain level: 5-7/10 during bowel movements, 3-5/10 at rest
What’s changing:
- Each bowel movement is less painful than the previous one
- You’re adjusting to the discomfort
- Swelling starts to decrease
- Discharge (blood-tinged fluid, mucus) is normal during healing
Activities:
- Continue rest at home (most patients still off work this week)
- Short walks outside (10-15 minutes, 2-3 times daily)
- Sitz baths continue 3-4 times daily
- Sleep is still difficult but improving
Medications:
- May start reducing pain medication frequency (but keep taking if needed)
- Continue stool softeners religiously
- Add fiber supplement if tolerated (psyllium, starting small doses)
Bowel movements:
- By day 5-7, bowel movements are still uncomfortable but
significantly better than day 2-3
- Aim for 1-2 soft bowel movements daily (neither constipation nor diarrhea)
Common concerns this week:
- “I’m still in pain—is this normal?” → Yes. Week 1 is the peak pain week.
- “I’m bleeding a little” → Small amounts of blood/discharge normal. Heavy bleeding is not.
- “I can’t sit at all” → Use donut cushion, limit sitting time, down when resting.
Week 2: The Turning Point (Days 8-14)
What’s Different:
Pain level: 3-5/10 during bowel movements, 2-4/10 at rest
Major improvement: This is when patients tell me “I turned a
corner.” Pain is still present but noticeably less than week 1.
Bowel movements:
- Much less anxiety about going
- Pain during is moderate rather than severe
- Recovery after is quicker
Activities:
- Desk work: Many patients return to office work end of week 2 (days 10-14)
- Light household tasks: Cooking, light cleaning (no heavy lifting)
- Driving: Can resume if off narcotic pain medication andn comfortable sitting for trip duration
- Walking: 20-30 minute walks twice daily
Medications:
- Transitioning to milder pain medication (paracetamol, ibuprofen if tolerated)
- Continue stool softeners (don’t stop just because you feel better)
- Fiber supplement now part of routine
Sitz baths:
- Continue 2-3 times daily minimum
- Especially important after bowel movements
Sleep:
- Improving significantly
- Most patients sleeping 5-7 hours at night
Healing:
- Wounds are closing (if open hemorrhoidectomy) or stitches dissolving (if closed)
- Discharge continues (normal)
- Slight bleeding or spotting when wiping (normal)
Week 3-4: Steady Progress (Days 15-28)
What’s Changing:
Pain level: 2-4/10 during bowel movements, 1-2/10 at rest
Daily life:
- Mostly back to normal daily activities
- Still avoiding heavy lifting, strenuous exercise
- Can sit for longer periods (1-2 hours with breaks)
Work:
- Desk jobs: Fully back to work
- Physical labor: Can return end of week 3 or during week 4 (depends on job demands)
- Avoid: Heavy lifting (>10-15 kg), prolonged standing without breaks
Bowel movements:
- Approaching normal (mild discomfort rather than pain)
- Frequency and consistency normalizing
- Still using stool softeners (continue through week 4)
Activities you can resume:
- Light exercise: Walking, gentle swimming (if wounds healed), stationary bike
- Light household chores: Laundry, dishes, vacuuming (avoid heavy furniture moving)
- Social activities: Dining out, short trips, seeing friends
Activities still to avoid:
- Heavy weightlifting or CrossFit
- Contact sports
- Very long car trips or flights
- Anything that significantly increases abdominal pressure
Sex:
- Can usually resume by week 3-4
- Go slowly, communicate with partner, stop if painful
- Use plenty of lubrication
Healing:
- Wounds mostly healed (80-90% closed)
- Discharge decreasing significantly
- Occasional spotting with wiping (still normal)
Week 5-6: Near Normal (Days 29-42)
What’s Changing:
Pain level: 1-2/10 during bowel movements, 0-1/10 at rest
Daily life:
- Feels nearly normal
- Most activities unrestricted (still cautious with very heavy lifting)
Bowel movements:
- Normal or near-normal
- Minimal to no discomfort
- Can gradually reduce or stop stool softeners (discuss with surgeon)
Activities you can resume:
- Moderate exercise: Jogging, light weights, yoga, Pilates
- Longer travel: Flights, road trips (bring cushion and stool softeners just in case)
- Most sports: Tennis, golf, swimming (full intensity)
Activities still to avoid:
- Very heavy deadlifts, squats with heavy weight
- Extreme straining exercises
Healing:
- 95% healed
- Minimal or no discharge
- Occasional mild itch as final healing occurs (normal)
Follow-up:
- Usually see surgeon for post-operative check around week Confirm healing is complete
- Discuss resuming all activities including heavy lifting
Week 7-8: Complete Healing (Days 43-56)
What’s Changing:
Pain level: 0-1/10, mostly or completely pain-free
Daily life:
- Back to 100% normal
- No restrictions
Activities:
- All activities unrestricted: Heavy lifting, intense exercise, contact sports
- Bowel movements: Completely normal
- No ongoing treatment needed (discontinue stool softeners if not needed for other reasons)
Healing:
- Complete
- Scars are minimal and continue to fade over months
Quality of life:
- Patients report: “I feel better than I have in years”
- Relief from bleeding, prolapse, discomfort
- No longer avoiding activities or feeling self-conscious
If symptoms persist or are not improving, a specialist assessment in Dubai can help determine the most appropriate treatment.
Pain Management Strategies That Actually Work
Medication Strategy:
Week 1:
- Strong pain medication: Take on schedule (every 4-6 hours), don’t wait until pain is severe
- Stool softeners: 2-3 times daily, non-negotiable
- Options: Tramadol, codeine/paracetamol combinations, NSAIDs if tolerated
Week 2:
- Transition to milder medication: Paracetamol, ibuprofen
- Continue stool softeners
Week 3-4:
- As-needed pain medication: Most patients need only occasional doses
- Continue stool softeners through week 4
Non-Medication Strategies:
Sitz Baths (Most Important Non-Drug Strategy):
- Warm (not hot) water, 10-15 minutes
- 3-4 times daily minimum (after each bowel movement + before bed)
- Add Epsom salts if desired (optional, not proven more effective but many patients like it)
- Helps: reduces pain, promotes healing, keeps area clean
Positioning:
- Avoid prolonged sitting: Sit <15-20 minutes at a time in week
- Use donut cushion: Reduces pressure on surgical area
- Lie down when resting: Better than sitting
Ice Packs:
- First 24-48 hours only
- Wrapped in cloth (never directly on skin)
- 15 minutes on, 15 minutes off
Topical Treatments:
- Lidocaine gel/cream for temporary numbing
- Diltiazem or nifedipine cream (relaxes anal sphincter, reduces pain during bowel movements)
The First Bowel Movement: Detailed Strategy
Since this is the #1 patient concern, here’s the complete strategy:
Preparation (Start Immediately After Surgery):
Stool Softeners:
- Docusate (Colace): 100-200mg twice daily
- Lactulose: 15-30ml once or twice daily
- Polyethylene glycol (Miralax): 17g daily in water
- Your surgeon will prescribe one or more of these
Hydration:
- 2.5-3 liters of water daily
- Avoid: caffeine, alcohol (dehydrating)
Food:
- Soft, easily digestible foods
- Prunes, pears, berries (natural laxative effect)
- Avoid: cheese, red meat, white bread (constipating)
When the Urge Comes (Usually Day 2-3):
Don’t delay. Holding it in makes stool harder.
Go to bathroom:
1. Take pain medication 30-60 minutes before if you can anticipate timing
2. Sit on toilet (don’t squat, don’t use footstool—normal sitting position)
3. Breathe slowly and deeply (anxiety increases muscle tension)
4. Let it happen naturally—don’t push, don’t strain, don’t hold breath
5. If nothing happens after 5 minutes, get up and try again when urge returns
During:
- Yes, it will sting/burn (7-9/10 pain for 2-5 minutes)
- This is expected and temporary
- Focus on breathing
Immediately After:
- Sitz bath (15 minutes, warm water)
- Apply topical anesthetic if prescribed
- Take pain medication if needed
- Rest for 30-60 minutes
Next bowel movements:
- Each one is easier than the last
- By day 5-7, significantly less painful
- By week 2-3, approaching normal
If You’re Constipated (No Bowel Movement by Day 4):
Contact your surgeon. You may need:
- Increased stool softener dose
- Suppository (glycerin or bisacodyl)
- Small enema (last resort)
Don’t let constipation persist—this makes everything worse.
Returning to Normal Activities: Specific Timeline
Driving:
- When: Off narcotic pain medication + comfortable sitting for duration of trip
- Typically: Week 2 for short trips, week 3-4 for longer drives
Work:
- Desk job (sedentary): Week 2 (days 10-14)
- Standing/walking job: Week 2-3
- Light manual labor: Week 3-4
- Heavy manual labor: Week 4-6
Exercise:
- Walking: Start immediately (day 1), increase gradually
- Swimming: Week 3-4 (once wounds healed)
- Light jogging: Week 4-5
- Weights (light): Week 4-5
- Heavy weights/CrossFit: Week 6-8
- Contact sports: Week 6-8
Sex:
- When: Week 3-4, or when comfortable
- Tips: Go slowly, communicate, use lubrication, stop if painful
Travel:
- Short flights (<3 hours): Week 3-4
- Long flights: Week 4-6
- Bring: Stool softeners, cushion, pain medication (just in case)
Gym/Sports:
- Avoid in week 1-3: Heavy lifting, exercises that significantly
increase abdominal pressure (squats, deadlifts, leg press with heav weight)
- Resume week 4-8: Gradually increase intensity
Warning Signs: When to Contact Your Surgeon
Most recovery is uncomplicated, but you should be aware of potential hemorrhoid complications and contact your surgeon if:
Urgent (Contact Immediately):
- Heavy bleeding: Soaking through dressings or toilet paper repeatedly
- Fever >38°C with increasing pain
- Inability to urinate for >12 hours
- Severe, uncontrolled pain despite medication
- Signs of infection: Increasing redness, swelling, pus discharge, foul odor
Non-Urgent (Contact Within 24 Hours):
- Constipation >4 days post-surgery
- Increasing pain after initial improvement
- Excessive drainage or discharge
- Concerns about healing
Normal (Don’t Worry):
- Mild to moderate pain (managed with medication)
- Small amount of blood/spotting when wiping (especially first 2-3 weeks)
- Mucus discharge during healing
- Occasional sharp twinges or spasms (healing nerves)
- Feeling like you need to have bowel movement even after going
(sensation normalizes over weeks)
Tips from Patients Who’ve Been Through It
Here’s advice from patients who’ve completed hemorrhoidectomy
recovery:
“I Wish I’d Known…”
1. “The anticipation was worse than reality”
- Many patients: “I was terrified, but it was manageable”
- Anxiety amplifies pain—realistic expectations help
2. “Stool softeners are MORE important than pain medication”
- Preventing hard stools prevents the worst pain
- Don’t skip doses even when you feel fine
3. “Week 2 felt like a miracle after week 1”
- Recovery is gradual but week 2 is noticeably better
- Knowing this helps you get through week 1
4. “I should have done this years ago”
- Most common patient comment at 3-month follow-up
- The recovery, while difficult, is temporary—the relief is permanent
5. “Sitz baths are your best friend”
- Patients who did 4-5 sitz baths daily reported better pain control than those who skipped them
Practical Tips:
Before Surgery:
- Stock up: stool softeners, pain medication, soft toilet paper (or use wipes), donut cushion, sitz bath basin
- Meal prep: make or buy easy meals for week 1-2
- Clear your schedule: take 2 weeks off work minimum
During Recovery:
- Set phone alarms for medication schedule (easy to forget when you’re uncomfortable)
- Keep a pain/bowel movement diary (helps track progress, shows you ARE improving)
- Don’t compare yourself to others (everyone’s recovery is slightly different)
- Celebrate small wins (first day without strong pain meds, first comfortable bowel movement, etc.)
Mindset:
- This is temporary (repeat this to yourself)
- It gets better every week
- You’re investing in long-term relief
Long-Term Outlook: Life After Recovery
3 Months Post-Surgery:
- Completely healed
- No pain, no restrictions
- Bowel movements normal
- Scars minimal/not noticeable
1 Year and Beyond:
- Recurrence rate: 5-10% (lowest of any hemorrhoid treatment)
- Most patients: “I haven’t thought about hemorrhoids in months—that’s how well I’m doing” Preventing Recurrence
- High-fiber diet (25-35g daily)
- Adequate hydration (2-3 liters daily)
- Don’t strain during bowel movements
- Don’t delay when you feel the urge
- Regular exercise
- Manage constipation proactively
This article is written and reviewed by Prof. Dr Antonio Privitera, consultant colorectal surgeon with fellowship training at Mayo Clinic (USA) and the Royal College of Surgeons (UK), specializing in hemorrhoid diagnosis and minimally invasive treatment.
Frequently Asked Questions
1. What if I can’t urinate after surgery?
Urinary retention occurs in 5-10% of patients (more common with spinal anesthesia). Usually resolves within 24 hours. Contact surgeon—you need temporary catheter.
2. Is bleeding normal during recovery?
Small amounts of blood/spotting when wiping are normal for first 2-3 weeks. Heavy bleeding (soaking through toilet paper repeatedly) is NOT normal—contact surgeon.
3. Can I take baths or only sitz baths?
Sitz baths (just hips/bottom submerged) are most effective. Full baths are okay after first week if wounds are healing well.
4. When can I stop stool softeners?
Usually week 4-6, but discuss with surgeon. Some patients continue them long-term if prone to constipation.
5. Will I be incontinent?
No. Temporary urgency or minor seepage can occur during healing but resolves in vast majority of patients within weeks to months.
6. How do I know if I have an infection?
Signs: fever, increasing pain (getting worse instead of better), pus discharge, spreading redness, foul odor. Contact surgeon if these develop.
7. Can I drink alcohol during recovery?
Avoid first 2-3 weeks (alcohol can irritate bowels, dehydrates, interacts with pain medication). Moderate alcohol okay after that.
8. What if pain is getting worse instead of better?
Contact surgeon. Possible causes: infection, abscess, excessive scar tissue. Usually treatable if caught early.
9. Is it normal to feel depressed during recovery?
Yes. Pain, limited activity, and discomfort can affect mood. Most patients feel much better emotionally by week 2-3 as pain improves. If depression persists, discuss with surgeon.
10. When will I feel “normal” again?
Most patients: “mostly normal” by week 4-6, “completely normal” by week 8. But you’ll notice significant improvement week by week from week 2 onward.
References and Medical Sources
This recovery guide is based on clinical experience and evidence:
1. American Society of Colon and Rectal Surgeons Guidelines – Post-operative care recommendations. Davis BR, Lee-Kong SA, Migaly J, Feingold DL, Steele SR. The American Society of Colon and Rectal Surgeons Clinical Practice Guidelines for the Management of Hemorrhoids. Dis Colon Rectum. 2018;61(3):284-292. PubMed
2. Pain Management After Hemorrhoidectomy – Evidence-based approaches. Joshi GP, Neugebauer EA; PROSPECT Collaboration. Evidence-based management of pain after haemorrhoidectomy surgery. Br J Surg. 2010;97(8):1155-68. PubMed
3. Post-operative Complications and Management – What to watch for. Simillis C, Thoukididou SN, Slesser AA, Rasheed S, Tan E, Tekkis PP. Systematic review and network meta-analysis comparing clinical outcomes and effectiveness of surgical treatments for haemorrhoids. Br J Surg. 2015;102(13):1603-18. PubMed
Medical Review: This content was written and reviewed by Professor training at the Mayo Clinic and Royal College of Surgeons (UK), and European Board Certification in Colorectal Surgery.
Post-Operative Support and Follow-Up
Recovering from hemorrhoidectomy? Have questions or concerns? Contact us for post-operative support.
📱 WhatsApp: +971 55 318 8469
📞 Phone: +971 55 318 8469
Dubai Locations:
- Medcare Medical Centre, Discovery Gardens
- Medcare Women and Children Hospital
- Medcare Royal Specialty Hospital
- Clemenceau Medical Centre
- Aster Hospital, Qusais
We’re here to support you through every stage of recovery.
Professor Dr. Antonio Privitera
Fellowship Training: Mayo Clinic | Royal College of Surgeons (UK)
European Board Certified in Colorectal Surgery
About the Author
