
Most simple anal fistulas are cured with one operation. But some fistulas – particularly complex ones, Crohn’s-related ones, or those that have failed multiple surgical attempts – require long-term management strategies rather than a single curative procedure. For full treatment approach, see anal fistula treatment in Dubai. This is not failure. It is an honest approach to a difficult condition.
When Is Long-Term Management Relevant?
- Crohn’s fistula that has not responded to surgery and medical treatment
- Very complex fistula involving most of the sphincter where cure is too risky for continence
- Multiple failed previous operations the anatomy is distorted and further surgery carries high risk
- Patient with poor sphincter function where any further division would cause incontinence
- Older patient who prefers quality of life over repeated surgery
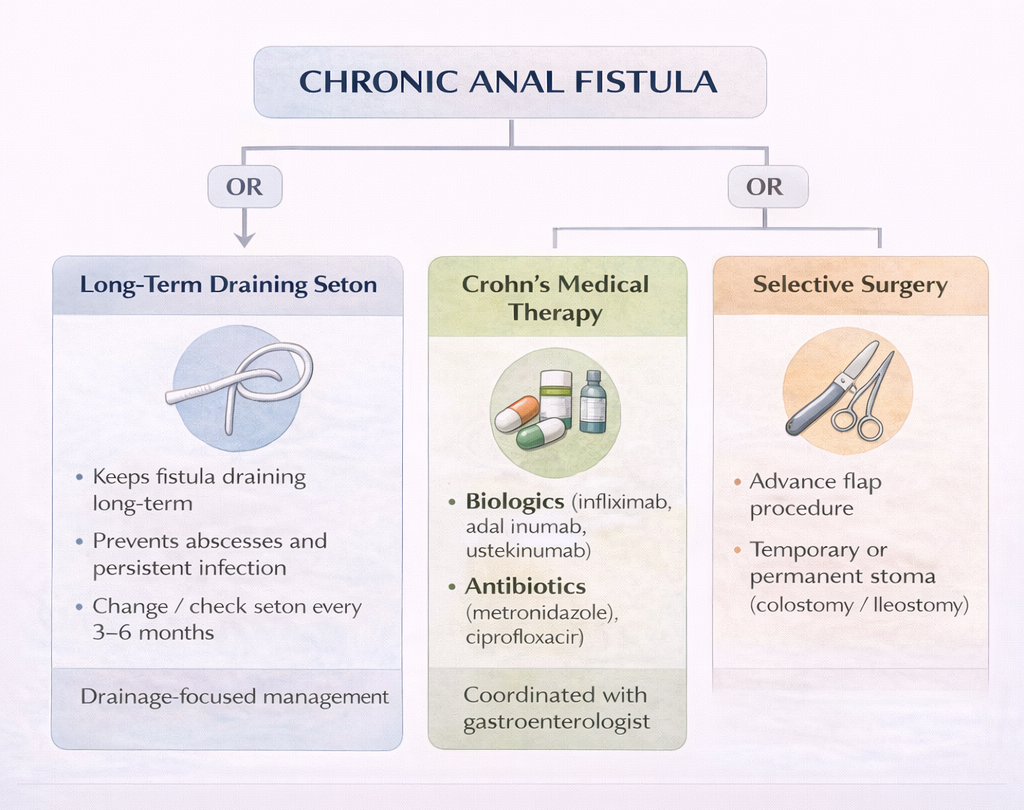
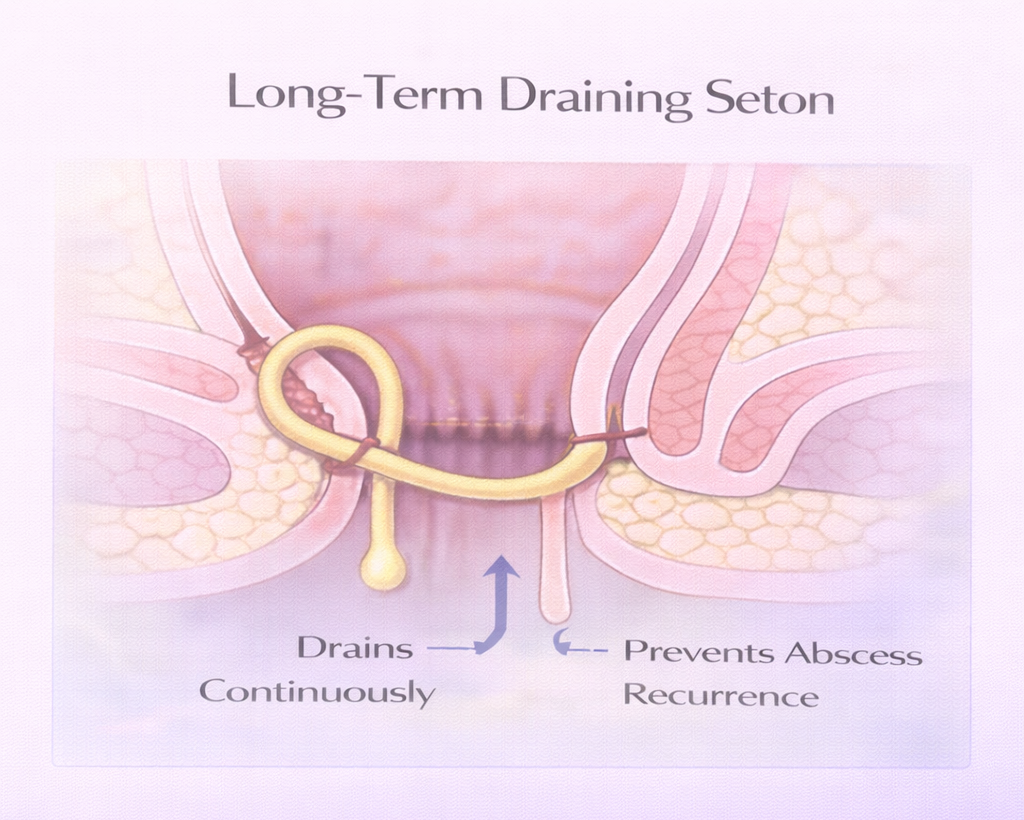
Strategy 1: Long-Term Draining Seton
A loose draining seton in Dubai keeps the fistula tract open permanently. This prevents recurrent abscess formation (the cycle of filling and painful swelling) while allowing ongoing drainage that the patient can manage.
- The seton must be maintained – replaced periodically
- Patients adapt well – most say the seton is much preferable to recurrent abscesses
- Suitable for: Crohn’s fistulas, complex fistulas where cure attempts have failed, patients who decline further curative surgery
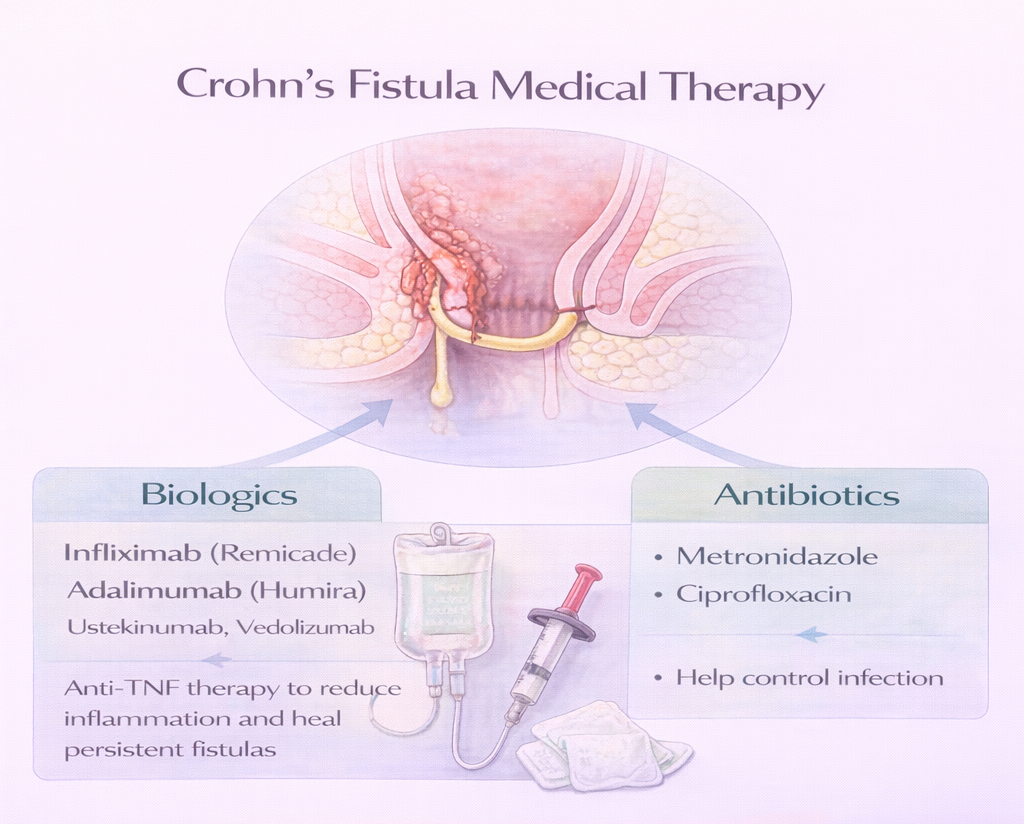
Strategy 2: Medical Treatment (Crohn’s Fistulas)
For Crohn’s-related fistulas, medical treatment plays a central role:
Biologics
- Infliximab (Remicade) – anti-TNF antibody: Best evidence for inducing fistula closure in Crohn’s. Closure rates of 30-55% with maintained dosing.
- Adalimumab (Humira): Alternative anti-TNF with similar efficacy
- Ustekinumab, vedolizumab: For patients who fail anti-TNF therapy
Antibiotics
- Metronidazole, ciprofloxacin: Can suppress discharge and control secondary infection but do not close fistulas
Important: Medical treatment in Crohn’s fistulas should be coordinated between the colorectal surgeon and the gastroenterologist.
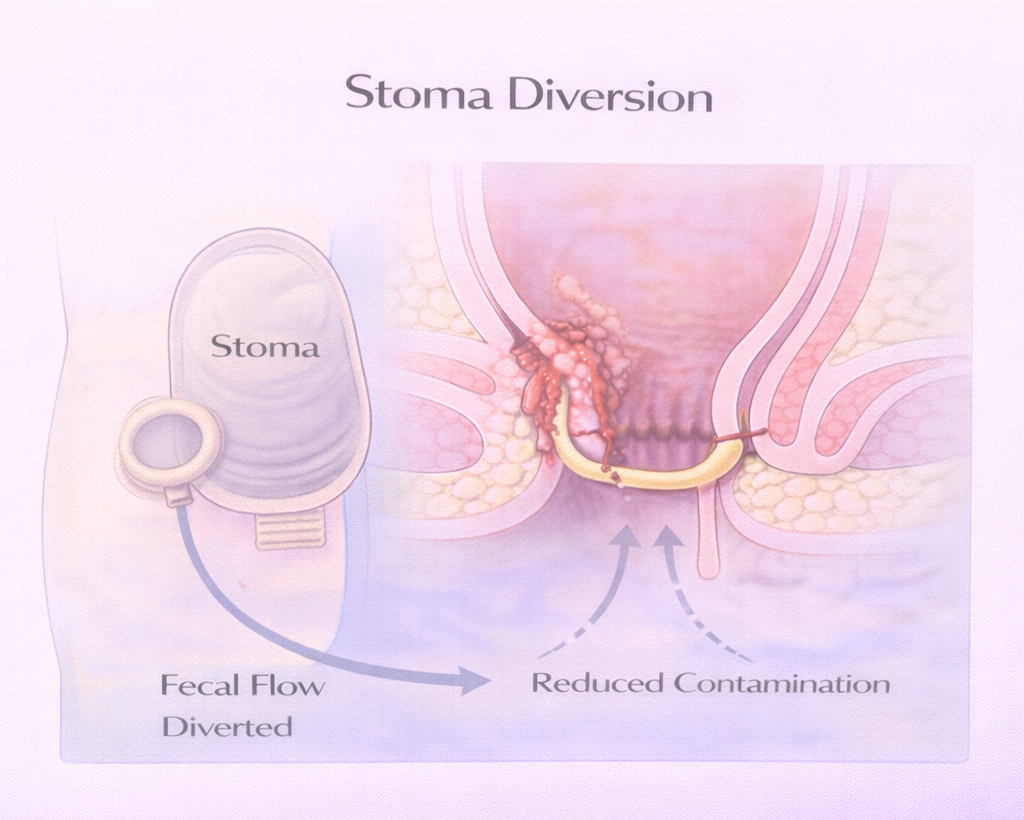
Strategy 3: Stoma (in Selected Cases)
A temporary or permanent defunctioning stoma (colostomy or ileostomy) diverts the fecal stream away from the anorectal area, reducing contamination and sometimes allowing a very complex fistula to heal or settle. Used when:
- Extensive Crohn’s perianal disease that cannot be controlled by other means
- Fistula associated with anorectal stricture or destroyed perineum
- Patient refuses seton but has recurrent sepsis
Quality of Life With Chronic Fistula
Living with a chronic fistula even a managed one affects quality of life:
- Discharge and soiling require pads socially restrictive
- Odor is a concern for many patients
- Pain during flare-ups
- Impact on sexual activity and relationships
These are legitimate concerns and should be discussed openly with your surgeon. There are practical strategies to improve quality of life at each stage:
- Barrier creams (zinc oxide) to protect perianal skin from constant moisture
- Appropriate absorbent pads
- Prompt treatment of any abscess flare-up to prevent a small collection becoming a large one
- Regular follow-up – fistulas that have been ‘stable’ can become complex over time
Need expert treatment for hemorrhoids, anal fissure, or anal fistula? Book a consultation with Dr. Antonio Privitera in Dubai or Abu Dhabi.
📱 WhatsApp: +971 55 318 8469
📞 Phone: +971 55 318 8469
AUTHOR AUTHORITY BLOCK
Fellowship-trained at Mayo Clinic (USA) and the Royal College of Surgeons (UK). Member of the Royal College of Surgeons of Edinburgh. Certified in General Surgery by the Italian Medical Council.
About the Author
