

Preventing hemorrhoid recurrence in Dubai requires lasting changes in bowel habits, diet, hydration, and lifestyle. Long-term success depends on treating both the hemorrhoids and the underlying causes, see our hemorrhoid treatment in Dubai. You’re recovered. Symptoms are gone. Now you’re wondering: Will they come back? What do I need to do to keep them from returning?
I’m Professor Dr. Antonio Privitera, Fellow of the American Society of Colon and Rectal Surgery and Fellow of the Royal College of Surgeons, the only surgeon in the world with both a Mayo Clinic and University of London Colorectal Surgery Fellowship, practicing across Dubai. The honest answer: Treatment removes or shrinks hemorrhoids, but
if you return to the habits that caused them, they can recur.
Recurrence rates vary by treatment:
- Banding: 10-30% recurrence over 5 years (higher for Grade III)
- Laser/THD: 10-20% recurrence
- Hemorrhoidectomy: 5-10% recurrence (lowest)
But here’s the good news: Most recurrence is preventable with consistent lifestyle habits.
This guide covers:
- Why hemorrhoids recur
- Post-treatment prevention strategies
- Long-term maintenance plan
- High-risk periods requiring extra vigilance
- When recurrence requires retreatment
For post-treatment follow-up:
Experiencing symptoms like these? A discreet same-day specialist assessment is available across.
WhatsApp: +971 55 318 8469 | Phone: +971 55 318 8469
Medcare Discovery Gardens (Dubai)
Why Hemorrhoids Recur
Treatment Removes Symptoms, Not Underlying Causes:
Hemorrhoid treatment addresses:
- The swollen hemorrhoidal tissue
- Prolapse
- Bleeding
Treatment does NOT address:
- Chronic constipation
- Straining habit
- Low-fiber diet
- Sedentary lifestyle
- Poor bathroom habits
If these underlying causes continue, new hemorrhoids can form.
Common Causes of Recurrence:
1. Return to Low-Fiber Diet
- You eat high-fiber immediately post-treatment
- Symptoms resolve
- Gradually slip back to old diet
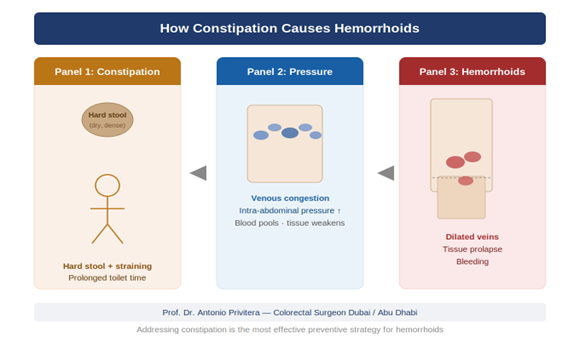
- Constipation returns → straining returns → hemorrhoids return
2. Inadequate Hydration
- Dubai climate requires more water
- You forget to drink enough
- Hard stools result
- Straining worsens
3. Bathroom Habits Revert
- Back to sitting 15 minutes on toilet with phone
- Delaying bowel movements when busy
- Straining
4. Life Changes
- Pregnancy
- New job (more sitting, less movement)
- Stress affecting bowel habits
- Travel
5. Incomplete Initial Treatment
- Treatment was appropriate but conservative (banding for Grade III when THD would have been better)
- Treating symptoms rather than addressing grade
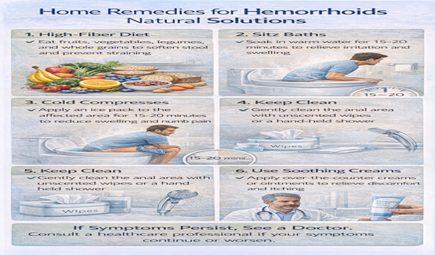
Core Prevention Strategies (The Non-Negotiables)
1. High-Fiber Diet (Forever)
Target: 25-35g fiber daily
Why it matters:
- Prevents constipation
- Softens stools
- Reduces need to strain
- Single most important prevention factor
How to maintain:
Make it habit, not effort:
- Breakfast: Always include fiber (oats, whole wheat bread, fruit)
- Lunch: Always include vegetables or salad
- Dinner: Same—vegetables with every meal
- Snacks: Fruits, nuts, dates instead of chips/biscuits
Fiber-rich foods readily available in Dubai:
- Dates (traditional, excellent fiber source)
- Hummus (chickpeas—high fiber)
- Lentils (عدس—very high fiber)
- Brown rice (substitute for white rice)
- Whole wheat bread (Arabic bread made with whole wheat)
- Fresh fruits (available year-round)
Fiber supplement if needed:
- Psyllium husk (Metamucil, Fybogel)
- Take daily if dietary fiber insufficient
- 1-2 tablespoons daily with water
2. Adequate Hydration (2.5-3 Liters Daily)
Why it matters:
- Fiber without water worsens constipation
- Dubai climate increases fluid needs
- AC environments reduce thirst sensation
How to maintain:
Set system, don’t rely on thirst:
- 1-liter bottle on desk, refill 2-3 times
- Glass of water with every meal
- Water before bed, upon waking
For every coffee: Drink equal amount of water
Signs you’re adequately hydrated:
- Urine is pale yellow
- Bowel movements are soft, formed
- Not feeling thirsty
3. Proper Bathroom Habits (Daily Discipline)
The rules:
Don’t delay when you feel urge:
- Go promptly
- Delaying leads to harder stools
5-minute maximum on toilet:
- Leave phone outside bathroom
- If nothing happens in 5 minutes, get up and try later
Don’t strain:
- If bowel movement doesn’t happen easily, don’t force it
- Increase fiber and water, try later
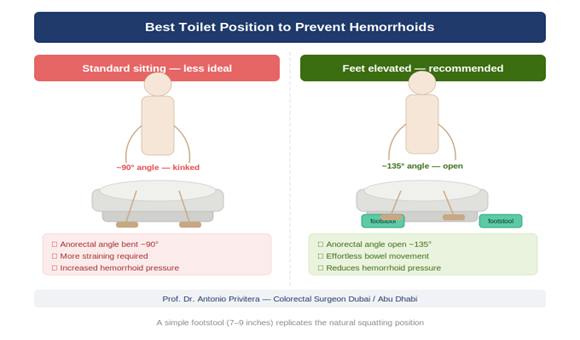
Use footstool:
- Elevate feet while sitting on toilet
- Opens anorectal angle
- Makes bowel movements easier
4. Regular Physical Activity
Why it matters:
- Promotes regular bowel movements
- Reduces sitting time
- Improves circulation
- Maintains healthy weight
Minimum: 30 minutes walking daily
Additional benefits:
- Breaks up sitting (office workers)
- Prevents constipation
- Reduces stress (stress affects digestion)
Dubai-appropriate:
- Walk in malls (climate-controlled)
- Early morning or evening outdoor walks
- Gym, swimming (year-round options)
Post-Treatment Timeline: What to Maintain When
First 3 Months (Critical Period):
Why critical:
- Hemorrhoids are healing/shrinking
- Establishing new habits
- Highest risk of slipping back to old patterns
What to do:
Diet:
- High fiber EVERY day (no exceptions)
- Fiber supplement if helpful
- Track fiber intake first month to establish baseline
Bowel habits:
- Stool softener if needed (especially post-surgery)
- Sitz baths as needed for comfort
- Strict 5-minute toilet rule
Activity:
- Walk daily
- Avoid very heavy lifting (depends on treatment type—follow surgeon’s guidelines)
Follow-up:
- Attend scheduled post-treatment appointment
- Report any symptoms immediately
Months 3-12 (Habit Formation):
Goal: Make prevention habits automatic
Diet:
- Continue high fiber (should feel natural by now)
- If you travel or slip for a few days, get back on track immediately
Bowel habits:
- Should be regular by now
- If constipation develops, address immediately (don’t let it become chronic)
Activity:
- Maintain regular exercise
Check-in:
- If symptoms return, see doctor early
- Don’t assume “it’s minor” and delay
Year 2+ (Long-Term Maintenance):
Goal: Prevention is lifestyle, not temporary effort
Continue all above:
- High fiber
- Hydration
- Good bathroom habits
- Regular activity
Annual check-up if:
- You had Grade III-IV hemorrhoids
- Multiple treatments
- Strong family history
Otherwise:
- See doctor if symptoms develop
- Don’t need routine hemorrhoid checks if asymptomatic
High-Risk Periods: Extra Vigilance Needed
Pregnancy:
If you’ve had hemorrhoids before, pregnancy high risk for recurrence.
Prevention:
- High fiber from week 1
- Hydration throughout
- Stool softeners if constipated
- Don’t delay bowel movements
- Gentle exercise (walking) throughout pregnancy
Delivery:
- Controlled pushing (follow midwife guidance)
- May still develop hemorrhoids despite prevention
Postpartum:
- Continue prevention strategies
- Stool softeners essential
- Most postpartum hemorrhoids improve with time
New Job/Life Change:
More sitting (new office job):
- Take movement breaks hourly
- Don’t sit through lunch
- Walk before/after work
Increased travel:
- Maintain fiber intake (harder while traveling)
- Bring fiber supplement
- Stay hydrated on flights
- Don’t delay bathroom breaks during meetings/flights
Increased stress:
- Stress affects digestion
- Maintain routines (diet, exercise, sleep)
- Manage stress (even 10 minutes daily helps)
Illness or Medication:
If prescribed medications that cause constipation:
- Pain medications (codeine, tramadol)
- Iron supplements
- Some antidepressants
Prevention:
- Stool softener alongside constipating medication
- Increase fiber
- Extra hydration
Aging:
As you age (50s, 60s+):
- Tissues weaken naturally
- More prone to constipation
- May need fiber supplement permanently
- Regular exercise becomes more important
When “Recurrence” Might Not Be Recurrence
Distinguish Between:
New hemorrhoids forming:
- You’ve returned to old habits
- New hemorrhoids develop
- This is true recurrence
Incomplete initial treatment:
- You were treated for Grade II but actually had Grade III
- Or treated with banding when THD would have been more definitive
- Symptoms persist or return quickly
Different problem:
- What you’re experiencing isn’t hemorrhoids
- Anal fissure, for example
- Needs re-evaluation
Skin tags:
- After hemorrhoid treatment, skin tags may remain
- These are cosmetic, not functional hemorrhoids
- Don’t require treatment unless bothersome
If symptoms return: Don’t assume recurrence without examination.
See doctor for proper assessment.
If symptoms persist or are not improving, a specialist assessment in Dubai can help determine the most appropriate treatment.
When to Consider Retreatment
Criteria for Retreatment:
Symptoms return and:
- Impact quality of life (pain, bleeding, prolapse)
- Conservative management doesn’t help
- Proper prevention efforts haven’t prevented recurrence
Options depend on initial treatment:
After banding:
- Can repeat banding if Grade I-II
- Consider THD or laser if Grade III
- Hemorrhoidectomy if Grade IV or multiple failed treatments
After laser/THD:
- Can repeat if appropriate
- Hemorrhoidectomy if more definitive treatment needed
After hemorrhoidectomy:
- True recurrence rare (5-10%)
- Usually new hemorrhoid formation at different location
- Can treat with banding if Grade I-II
Discuss with surgeon:
- Why recurrence occurred
- Whether prevention strategies were followed
- Best treatment option going forward
Special Considerations for Dubai Residents
Climate Challenges:
Hot weather (summer months):
- Increased dehydration risk
- Need 3+ liters water daily
- AC environments mask thirst
Travel frequency:
- Many Dubai residents travel often for work
- Maintain fiber intake while traveling (challenging but important)
- Pack fiber supplement
Dietary Culture:
Eating out frequently:
- Choose high-fiber options when possible
- Salads, hummus, lentil dishes, whole wheat bread
- Avoid exclusively low-fiber meals (white rice, pasta, fried foods)
Traditional foods:
- Many Middle Eastern foods are high-fiber (lentils, chickpeas, dates)
- Use these to your advantage
Lifestyle Factors:
Office culture:
- Long sitting hours common
- Make conscious effort to move
- Walk during lunch break
Gym culture:
- Heavy weightlifting popular in Dubai gyms
- Use proper form
- Don’t hold breath during lifts
- If you’ve had hemorrhoids, consider lighter weights/more reps
This article is written and reviewed by Prof. Dr Antonio Privitera, consultant colorectal surgeon with fellowship training at Mayo Clinic (USA) and the Royal College of Surgeons (UK), specializing in hemorrhoid diagnosis and minimally invasive treatment.
Frequently Asked Questions
1. If I follow all prevention strategies, will hemorrhoids never come
back?
Prevention dramatically reduces risk but doesn’t guarantee 100%. Lifefactors (pregnancy, aging, illness) can still contribute. But good habits minimize risk significantly.
2. How long do I need to maintain prevention habits?
Forever. These aren’t temporary measures—they’re healthy lifestyle habits that benefit overall health, not just hemorrhoid prevention.
3. Can I stop fiber supplement once symptoms are gone?
If you’re eating 25-35g fiber from food daily, yes. If not, continue supplement. Many people find supplement easier than tracking dietary fiber.
4. What if I slip back to old habits for a few weeks?
Get back on track immediately. A few weeks won’t necessarily cause recurrence, but prolonged return to old habits will.
5. Do I need annual hemorrhoid check-ups?
Not if asymptomatic. But if you had Grade III-IV, annual colorectal health check is reasonable. Otherwise, see doctor only if symptoms develop.
6. If hemorrhoids recur, does that mean my treatment failed?
Not necessarily. Treatment was successful but prevention habits may not have been maintained. Or new life factors contributed (pregnancy, new job, etc.).
7. Can stress cause hemorrhoids to come back?
Stress affects digestion and bowel habits, which can contribute to hemorrhoids. Managing stress is part of overall prevention.
8. Is it normal to have occasional minor symptoms?
Occasional mild discomfort or tiny amount of bleeding can happen. If brief and resolves quickly, not necessarily recurrence. If persists, see doctor.
9. Should I avoid certain foods forever?
No specific foods cause hemorrhoids. The key is adequate fiber and hydration. You don’t need to avoid spicy food, coffee, etc. Just balance with fiber and water.
10. What if I travel frequently for work?
More challenging but manageable. Bring fiber supplement, choose high-fiber meals when possible, stay hydrated on flights, don’t delay bathroom breaks.
The Bottom Line: Prevention Is Simpler Than Treatment
Consider the effort:
Treatment:
- Office visit, procedure, recovery time, cost
Prevention:
- Daily fiber, water, 30-minute walk, proper bathroom habits
Prevention is less effort than retreatment.
Most patients tell me: “I wish I’d prevented this in the first place. Now that I know how, I’m not going back to old habits.”Make prevention non-negotiable like brushing your teeth—daily habit that becomes automatic.
References and Medical Sources
1. Hemorrhoid Recurrence Rates – Long-term outcomes. Simillis C, Thoukididou SN, Slesser AA, Rasheed S, Tan E, Tekkis PP. Systematic review and network meta-analysis comparing clinical outcomes and effectiveness of surgical treatments for haemorrhoids. Br J Surg. 2015;102(13):1603-18. PubMed
2. Dietary Fiber and Prevention – Evidence for long-term prevention. Alonso-Coello P, Mills E, Heels-Ansdell D, et al. Fiber for the treatment of hemorrhoids complications: a systematic review and meta-analysis. Am J Gastroenterol. 2006;101(1):181-8. PubMed
3. Lifestyle Modification Effectiveness – Prevention strategies. Garg P, Singh P. Adequate dietary fiber supplement and TONE can help avoid surgery in most patients with advanced hemorrhoids. Minerva Gastroenterol Dietol. 2017;63(2):92-96. PubMed
Medical Review: This content was written and reviewed by Professor Dr. Antonio Privitera, Fellow of the American Society of Colon and Rectal Surgery and Fellow of the Royal College of Surgeons, the only Colorectal Surgery Fellowship.
Post-Treatment Follow-Up and Long-Term Care
We support you beyond initial treatment with prevention guidance and monitoring.
Experiencing symptoms like these? A discreet same-day specialist assessment is available across Dubai.
WhatsApp: +971 55 318 8469 | Phone: +971 55 318 8469
Medcare Discovery Gardens (Dubai)
Dubai Locations
Multiple convenient locations for follow-up care
Long-term success through prevention and monitoring.
Professor Dr. Antonio Privitera
Operative Requirements:
Blood tests: Required before procedures with anesthesia
ECG: Required for patients over certain age or with cardiac history
Medical clearance: From cardiologist or internist if health conditions present
These typically not included in quoted procedure price.
Post-Operative Medications:
Pain medication: Usually 3-7 days supply
Stool softeners: 2-4 weeks supply
Topical treatments: Cream, ointments
Antibiotics: If prescribed (not always needed)
Total medication costs typically modest but add to overall expense.
Time Off Work:
Indirect cost—lost wages:
- Banding: 1-2 days
- Laser/THD: 5-10 days
- Hemorrhoidectomy: 10-21 days (depending on job type)
Factor this into total “cost” of treatment when comparing options.
Follow-Up Care:
Routine follow-up: Usually included in package price
Unscheduled visits: For complications, concerns may incur additional charges
Extended follow-up: Beyond initial healing period may have separate charges
Insurance Coverage Considerations
What Insurance Typically Covers:
Medically necessary treatment:
- Consultation and diagnosis
- Treatment appropriate for hemorrhoid grade
- Conservative measures tried first (when appropriate)
- Post-operative care
Pre-authorization required for:
- All procedures (banding, laser, THD, surgery)
- Submit 3-5 business days before procedure
- Approval confirms coverage
What Insurance May NOT Cover:
Cosmetic procedures:
- Removal of asymptomatic skin tags
- Treatment requested solely for appearance
“Elective” by insurer definition:
- Grade I-II hemorrhoids that haven’t tried conservative treatment
- Treatment insurer deems “not medically necessary”
Out-of-network providers:
- Some plans don’t cover or have high out-of-pocket
- Always verify network status
Maximizing Insurance Coverage:
Steps to take:
1. Verify your coverage before consultation
2. Choose in-network provider
3. Get proper referral if required
4. Try conservative treatment first (fiber, hydration) and document
5. Ensure surgeon’s office handles pre-authorization
6. Keep documentation of all symptoms, impact on life
See Day 23 article for detailed insurance guidance.
Payment Options
Insurance Direct Billing:
How it works:
- Facility bills insurance directly
- You pay copay/deductible only
- Remaining balance settled between provider and insurer
Advantage: Easiest for patient, lowest out-of-pocket
Requirement: Must be in-network, pre-authorized
Self-Pay (No Insurance):
Payment methods accepted:
- Credit card
- Bank transfer
- Cash (some facilities)
- Medical financing (some facilities offer)
Advantage: No insurance approval needed, immediate scheduling
Disadvantage: Full cost upfront
Payment Plans:
Some facilities offer:
- Installment payments
- Interest-free periods
- Credit arrangements
Eligibility: Varies by facility
Terms: Typically 3-12 months
Medical Tourism Considerations:
Some Dubai residents travel to home country:
- India, Philippines, UK, Europe for treatment
- May be less expensive
- Consider travel costs, time off, follow-up logistics
Or expats come to Dubai for treatment:
- UAE offers excellent quality care
- Prices competitive regionally
- English widely spoken
Value vs Price: What You’re Paying For
Why Cheapest Isn’t Always Best:
Surgeon qualifications matter:
- Fellowship-trained colorectal surgeon brings specialized expertise level
- Experience with full range of treatments ensures appropriate recommendation
Facility quality matters:
- Accreditation standards
- Complication management capability
- Equipment quality
Comprehensive care matters:
- Proper diagnosis (not just symptom treatment)
- Appropriate treatment for YOUR grade
- Post-operative support
- Accessibility for questions/concerns
Red Flags for Pricing:
Too cheap:
- May indicate less experienced surgeon
- May indicate hidden costs
- May indicate “assembly line” approach
Unclear pricing:
- Won’t quote costs upfront
- Vague about what’s included
- Surprise bills after treatment
Pressure tactics:
- Must decide today to get this price
- Discounts if you book now
- Aggressive marketing
Good practice:
- Transparent pricing
- Clear breakdown of included services
- Written estimate before proceeding
- No pressure to decide immediately
Comparing Treatment Options by Cost-Effectiveness
Grade I-II Hemorrhoids:
Best value: Banding
- Effective for this grade
- Office procedure (no OR costs)
- Minimal recovery (no lost wages)
- Total investment includes 2-3 sessions
- Recurrence rate acceptable for Grade I-II
Overspending: Surgery
- Unnecessary for this grade
- Higher cost, longer recovery
- Same outcome as banding
Grade III Hemorrhoids:
Best value: THD or Laser
- Single procedure
- Less invasive than surgery
- Good long-term results
- Moderate recovery time
Underspending: Banding
- May work but higher recurrence for Grade III
- May need repeat treatments
- Total cost of multiple sessions adds up
Overspending: Surgery
- Works, but more invasive than needed
- Unless multiple failed treatments
Grade IV Hemorrhoids:
Best value: Hemorrhoidectomy
- Most definitive treatment
- Lowest recurrence
- Worth the investment for permanent solution
Underspending: Banding or laser
- Won’t work for Grade IV
- Wasted money on ineffective treatment
Getting Accurate Quotes
Questions to Ask:
About the quote:
1. “What exactly is included in this price?”
2. “What additional costs should I expect?”
3. “Does this include follow-up visits?”
4. “Are medications included?”
5. “What if complications occur—what’s covered?”
6. “Will you handle insurance pre-authorization?”
7. “Do you accept direct billing?”
8. “What will my out-of-pocket be after insurance?”
9. “Are you in my insurance network?”
10. “What payment methods do you accept?”
11. you offer payment plans?”
12. “When is payment due?”
Get It in Writing:
Request:
- Detailed written estimate
- Itemized breakdown
- Insurance coverage confirmation (after pre-auth)
- Payment terms if applicable
Don’t proceed without clear understanding of total cost.
Dubai Pricing
General Observations:
Dubai:
- Wide range of pricing
- Premium areas (Marina, Downtown) tend higher
- More competition may offer more options
Dhabi:
- Comparable pricing to Dubai
- Government facilities may have different structure
- Insurance coverage good (Daman, Thiqa)
Both cities offer:
- Excellent quality care
- Fellowship-trained surgeons
- Modern facilities
Price shouldn’t be only factor in choosing city—choose based on
surgeon and convenience.
Frequently Asked Questions
1. Why do prices vary so much between facilities?
Overhead costs, surgeon experience, facility type, included services, and insurance contracts all affect pricing. Higher isn’t always better, but significantly lower may indicate quality concerns.
2. Can I negotiate medical prices in Dubai?
Some facilities offer package deals or discounts for self-pay patients. Worth asking, especially if paying cash. Insurance-negotiated rates are fixed.
3. Is hemorrhoid treatment tax-deductible in UAE?
UAE has no income tax, so medical expense deductions don’t apply. But in your home country (if you’re expat), may be deductible—consult advisor.
4. What if I can’t afford treatment?
Discuss payment plans with facility. Some offer charitable care. Don’t delay treatment—early treatment is less expensive than advanced disease.
5. Does price include revision if treatment fails?
Usually not. Repeat procedures incur additional charges. Ask about policies upfront.
6. Should I shop around for lowest price?
Get 2-3 quotes to understand market rate. But prioritize surgeon qualifications and facility quality over price alone.
7. What’s included in “comprehensive package”?
Ask specifically. Should include: surgeon, anesthesia, facility, basic follow-up. May not include pre-op tests, medications, extended follow-up.
8. Can I use FSA/HSA?
If you have US-based flexible spending account or health savings account, medical expenses abroad may be eligible. Check your plan rules.
9. Will my employer know if I use company insurance?
Your employer will know you used insurance but not specific medical details (HIPAA/privacy laws protect diagnosis).
10. What if I’m quoted different prices by same surgeon at different locations?
Facility fees vary by location. Surgeon fee may be same, but hospital vs clinic charges differ.
The Investment in Quality of Life
Consider the Real Value:
You’re not just paying for a procedure—you’re paying for:
- End to embarrassing symptoms
- Ability to sit comfortably again
- No more bleeding, pain, prolapse
- Return to normal activities
- Peace of mind (proper diagnosis)
- Professional expertise and safety
Perspective:
- How much have you spent on ineffective creams over months/years?
- How many work days have you lost to symptoms?
- What’s your quality of life worth?
Most patients say: “I wish I’d done this sooner. The cost was worth it.”
References and Medical Sources
1. Healthcare Pricing Transparency – Consumer information. Dubai Health Authority pricing guidelines. DHA Healthcare Pricing
2. Cost-Effectiveness of Hemorrhoid Treatments – Value analysis. Garg P. Conservative treatment, office-based procedures, or surgery for hemorrhoidal disease: an economic analysis. World J Gastrointest Surg. 2016;8(11):711-717. PubMed
Medical Review: This content was written and reviewed by Professor Dr. Antonio Privitera, Fellow of the American Society of Colon and Rectal Surgery and Fellow of the Royal College of Surgeons, the only Colorectal Surgery Fellowship.
Transparent Pricing and Insurance Support
We provide clear cost estimates and help navigate insurance coverage.
Experiencing symptoms like these? A discreet same-day specialist assessment is available across Dubai .
WhatsApp: +971 55 318 8469 | Phone: +971 55 318 8469
Medcare Discovery Gardens (Dubai)
Our Commitment:
- Transparent pricing upfront
- Insurance verification before treatment
- Written estimates
- No surprise bills
- Payment plans available for self-pay
About the Author
