
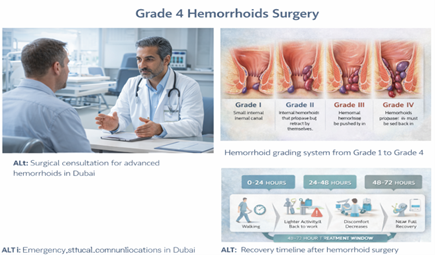
Grade 4 hemorrhoids in Dubai are the most advanced form and usually require specialist procedural or surgical treatment. Early assessment helps reduce complications and define the most effective option. Our hemorrhoid treatment in Dubai explains all grade-based options. other treatments—banding, creams, dietary changes—and they haven’t worked. Or perhaps your hemorrhoids are permanently prolapsed (hanging outside the anus and won’t go back in) and you’re finally seeking help after months or years of putting it off.
Here’s the reality: Grade IV hemorrhoids almost always require surgery. Not because surgeons want to do surgery, but because less invasive treatments (banding, laser, even THD) simply don’t work for Grade IV disease. The hemorrhoid tissue is too prolapsed, too large, and often includes both internal and external components.
Surgery—specifically hemorrhoidectomy (surgical removal)—is the only treatment that reliably works.
I’m Professor Dr. Antonio Privitera, a consultant colorectal surgeon with fellowship training at the Mayo Clinic and Royal College of Surgeons (UK), practicing across Dubai. I perform hemorrhoidectomy regularly, and I also perform all the less invasive options (banding, laser, THD). When I recommend surgery, it’s because it’s the right match for your anatomy—not because it’s the only thing I do.
This article explains:
- What Grade IV hemorrhoids are (and why they need surgery)
- What hemorrhoidectomy actually involves
- Honest recovery timeline (not sugarcoated)
- Pain management strategies
- When to consider surgery even for Grade III
- Why delaying surgery often makes things worse
Experiencing symptoms like these? A discreet same-day specialist assessment is available across Dubai
WhatsApp: +971 55 318 8469 | Phone: +971 55 318 8469
Medcare Discovery Gardens (Dubai)
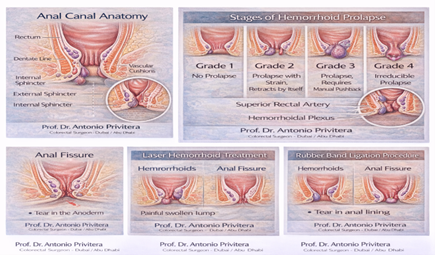
What Are Grade IV Hemorrhoids?
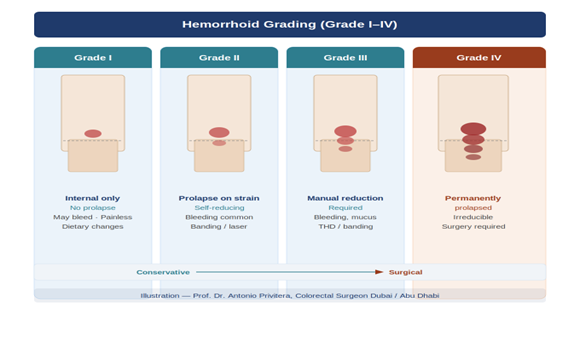
Hemorrhoids are graded I through IV based on prolapse (how much they come out of the anus):
- Grade I: Bleed but don’t prolapse
- Grade II: Prolapse during straining, go back in automatically
- Grade III: Prolapse during bowel movements, require manual reduction (you push them back in)
- Grade IV: Permanently prolapsed and cannot be reduced (pushed back in)
Grade IV hemorrhoids:
- Stay outside the anus all the time
- Cannot be pushed back inside
- Often include large external components
- May have skin tags, inflammation, and chronic irritation
- Cause significant symptoms: bleeding, mucus discharge, discomfort, difficulty cleaning, embarrassment
For more on hemorrhoid grading, see our comprehensive hemorrhoid treatment guide.
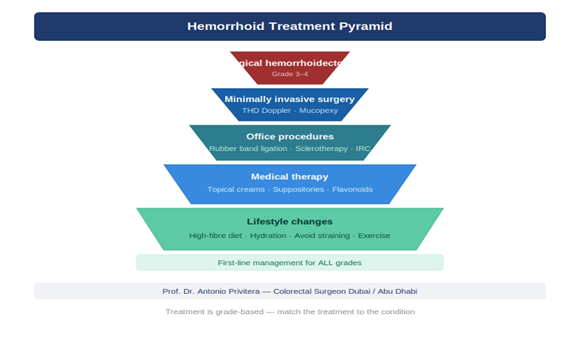
Why Grade IV Hemorrhoids Need Surgery
Here’s why less invasive treatments don’t work for Grade IV:
Rubber Band Ligation (Banding) – Won’t Work
- Banding treats internal hemorrhoids by cutting off blood supply
- Grade IV hemorrhoids are permanently prolapsed with large external components
- Banding can’t address the prolapsed tissue or external components
- Attempting banding on Grade IV sets you up for failure and frustration
Laser Hemorrhoidoplasty – Insufficient
- Laser shrinks internal hemorrhoid tissue from inside
- Grade IV hemorrhoids are too large and too prolapsed for laser alone to be effective
- Laser doesn’t address external components or skin tags
- You’ll waste AED 15,000-25,000 and still need surgery
THD (Transanal Hemorrhoidal Dearterialization) – Limited Role
- THD can work for some Grade IV cases if the external component is minimal
- But most Grade IV hemorrhoids have significant external tissue that THD can’t address
- Success rate for THD in Grade IV is much lower than for Grade II-III
Hemorrhoidectomy – The Definitive Solution
- Surgically removes both internal and external hemorrhoid tissue
- Addresses all components: prolapsed internal hemorrhoids, external hemorrhoids, skin tags
- Provides permanent relief in most cases
- Highest success rate and lowest recurrence of any treatment
Bottom line: If you have Grade IV hemorrhoids, surgery is almost
always necessary. Attempting less invasive treatments first usually
delays the inevitable while you continue suffering symptoms.
When Surgery Is Also Considered for Grade III
Grade III hemorrhoids (prolapse and require manual reduction) are a gray
zone:
Try Less Invasive First:
- Many Grade III hemorrhoids respond well to THD or laser
- If the external component is small, these are worth trying first
Consider Surgery If:
- THD or laser has failed
- Large external component is present
- You want the most definitive treatment with lowest recurrence
- Symptoms are severe and significantly impacting quality of life
Discuss options with your surgeon. Some patients with Grade III prefer to try THD first (knowing surgery is backup if needed). Others prefer to go straight to surgery for definitive treatment.
What Is Hemorrhoidectomy? The Procedure Explained
Hemorrhoidectomy is the surgical removal of hemorrhoid tissue. Here’s what happens:
Pre-Operative:
- You’ll have pre-operative assessment (blood tests, medical clearance)
- Stop blood thinners if you’re on them (with cardiologist approval)
- Bowel preparation is usually NOT required (unlike colonoscopy)
- You’ll be admitted day-of-surgery (typically day-case—home the same day, or overnight stay)
Anesthesia:
- Spinal anesthesia (numbs lower body, you’re awake but feel nothing) O General anesthesia (fully asleep)
The Surgery (30-60 minutes):
Positioning: You’re positioned for access to the anal area
Excision: I identify each hemorrhoid complex (usually 3 mai positions) and:
1. Carefully dissect and remove the hemorrhoid tissue
2. Ligate (tie off) the blood vessels feeding the hemorrhoid
3. Either leave the wound open to heal naturally (ope hemorrhoidectomy / Milligan-Morgan) or stitch it closed (close hemorrhoidectomy / Ferguson)
Technique variations:
- Traditional: Using scalpel and electrocautery
- LigaSure or Harmonic scalpel: Energy devices that seal vessels as they cut (less bleeding)
- Laser-assisted: Using laser for cutting (marketed as “less painful” but evidence is mixed)
Open vs Closed:
- Open (Milligan-Morgan): Wounds left open, heal naturally over 4-6 weeks. Less postoperative complications (abscess/infection) but longer healing.
- Closed (Ferguson): Wounds stitched closed, faster healing but slightly higher risk of complications.
Both techniques have similar long-term outcomes. I choose based on hemorrhoid characteristics and patient factors.
Recovery Room:
- You’ll wake up in recovery with pain medication on board
- Once stable and able to urinate, you go home (or to ward if overnight stay)
- Pain medication, stool softeners, and post-op instructions provided
Recovery Timeline: The Honest Truth
Let me be direct: hemorrhoidectomy recovery is uncomfortable. It’s the most painful of all hemorrhoid treatments. But with proper expectations and pain management, it’s manageable—and the long-term relief is worth it.
Week 1: The Hardest Week
Days 1-3: Most Painful
- Pain level: 6-8 out of 10 (with medication)
- What you’ll feel: Throbbing pain, discomfort, anxiety about first bowel movement
- Medications: Strong pain medication (tramadol, codeine, or occasionally opioids), stool softeners, laxatives
- Activities: Rest at home, sitz baths 3-4 times daily, minimal movement
- First bowel movement: Usually day 2-3. This is what patients fear most. Yes, it will be uncomfortable, but using stool softeners and not delaying makes it manageable. Pain improves with each subsequent bowel movement.
Days 4-7: Gradual Improvement
- Pain level: 4-6 out of 10
- Bowel movements: Still uncomfortable but less so than first one
- Activities: Short walks encouraged, still mostly resting at home
- Most patients: Still off work this week
Week 2: The Turning Point
- Pain level: 3-5 out of 10
- What changes: Pain decreases significantly, bowel movements become less scary
- Medications: Transitioning to milder pain medication (paracetamol, ibuprofen if tolerated)
- Return to work: Many patients with desk jobs return by end of week 2
- Physical work: Not yet—still need another 1-2 weeks
Weeks 3-4: Steady Improvement
- Pain level: 1-3 out of 10
- Activities: Light activities resume, still avoiding gym/heavy lifting
- Healing: Wounds are healing well, less discharge/spotting
- Physical work: Can usually resume by week 3-4
Weeks 6-8: Full Recovery
- Pain: Resolved or minimal
- Healing: Complete
- Activities: Unrestricted, including exercise and heavy lifting
- Follow-up: Check-in with surgeon to confirm healing
If symptoms persist or are not improving, a specialist assessment in Dubai can help determine the most appropriate treatment.
Common Timeline Questions:
“When can I drive?”
- When you’re off narcotic pain medication (usually week 2)
“When can I return to gym?”
- Light cardio (walking, swimming): Week 2-3
- Weights and strength training: Week 4-6
- Heavy lifting: Week 6-8
“When can I travel?”
- Short trips: Week 2-3
- Long flights: Week 3-4 (bring cushion, stool softeners)
Pain Management: How We Keep You Comfortable
Modern pain management has made hemorrhoidectomy recovery much more
tolerable than it was 20 years ago:
Immediate Post-Op:
- Long-acting local anesthetic injected around surgical site during surgery (provides 12-24 hours of pain relief) IV or oral pain medication before you leave hospital
At Home (Week 1-2):
Pain medication:
- Strong analgesics (tramadol, codeine, paracetamol combinations)
- NSAIDs if tolerated (ibuprofen reduces inflammation and pain)
- Short course of opioids if needed (morphine, oxycodone) for severe pain
Stool management (CRITICAL):
- Stool softeners (docusate, lactulose): Start immediately, use for 2-4 weeks
- Fiber supplements (psyllium): Start when comfortable
- Goal: Soft, formed stools that pass easily without straining
Sitz baths:
- Warm (not hot) water for 10-15 minutes, 3-4 times daily
- Especially helpful after bowel movements
- Soothes pain and keeps area clean
Topical treatments:
- Lidocaine gel for temporary numbing
- Diltiazem or nifedipine cream (relaxes anal sphincter, reduces pain)
At Home (Week 2-4):
- Transition to milder pain medication
- Continue stool softeners
- Continue sitz baths as needed
Complications and What to Watch For
Hemorrhoidectomy is generally safe, but complications can occur:
Common (5-10% of patients):
- Urinary retention: Difficulty urinating after surgery (more common with spinal anesthesia). Usually resolves within 24 hours; may require temporary catheter.
- Constipation: Fear of pain causes patients to avoid bowel movements. Don’t delay—this makes things worse. Use stool softeners as prescribed.
- Bleeding: Minor bleeding or spotting during healing is normal.
Heavy bleeding is rare but requires evaluation.
Uncommon (<5%):
- Infection or abscess: Fever, increasing pain, pus discharge.
Requires antibiotics, sometimes drainage.
- Anal stenosis (narrowing): Too much tissue removed or excessive scarring. Can usually be managed with dilation or minor procedure.
- Fecal incontinence or urgency: Usually temporary, resolves within weeks to months.
When to Seek Urgent Care:
- Heavy bleeding (soaking through dressings)
- Fever (>38°C) with worsening pain
- Inability to urinate for more than 12 hours
- Severe, uncontrolled pain despite medication
Success Rates and Recurrence
Hemorrhoidectomy has:
- High symptom relief: 90-95% of patients report significant improvement
- Low recurrence: 5-10% over 5-10 years (lowest of any hemorrhoid treatment)
- High patient satisfaction: Despite difficult recovery, most patients say “I wish I’d done this sooner”
Recurrence is usually due to:
- Not addressing underlying causes (chronic constipation, straining)
- New hemorrhoid formation (different from original)
Maintaining good bowel habits (fiber, hydration, no straining) minimize recurrence risk.
Why Patients Delay Surgery (And Why That’s Usually a Mistake)
Common reasons patients delay hemorrhoidectomy:
“I’m scared of the pain”
Reality: Yes, recovery is uncomfortable. But Grade IV hemorrhoid cause chronic daily discomfort, bleeding, hygiene issues, embarrassment.
Most patients tell me afterward: “I should have done this year ago—the recovery was tough but temporary, and now I’m finally fre this problem.”
“I’m too busy with work”
Reality: You need 7-14 days off work. That feels like a lot. But how many days have you spent uncomfortable, dealing with bleeding, or limiting activities because of hemorrhoids? Surgery gives you permanent relief.
“I heard hemorrhoid surgery is the most painful surgery”
Reality: It IS one of the more uncomfortable recoveries. But modern pain management, stool softeners, and proper expectations make it manageable. And the alternative—living with Grade IV hemorrhoids indefinitely—is often worse.
“Maybe it will get better on its own”
Reality: Grade IV hemorrhoids don’t improve on their own. The tissue is permanently prolapsed. Delaying surgery often makes things worse as hemorrhoids can become more inflamed, develop complications (thrombosis, strangulation), or cause chronic anemia from bleeding.
My Approach: When I Recommend Surgery
I don’t recommend hemorrhoidectomy lightly. If your hemorrhoids can be treated with banding or THD, I’ll recommend those first. But here’s
when I recommend surgery:
Clear Indications for Hemorrhoidectomy:
- Grade IV hemorrhoids (permanently prolapsed, can’t be reduced)
- Large Grade III hemorrhoids with significant external component
- (THD/laser unlikely to work)
- Mixed hemorrhoids (internal + external) causing significant symptoms
- Failed less invasive treatments (banding, laser, THD tried and symptoms persist)
- Complications (recurrent thrombosis, chronic bleeding causing anemia, strangulation)
Patient Decision After Full Discussion:
Some Grade III patients choose surgery after I explain:
- THD/laser might work (60-80% success)
- Surgery has higher success and lower recurrence (90-95%)
- Recovery: THD 1 week, surgery 2-4 weeks
- Cost is similar
I support either choice—but I’m honest about trade-offs.
This article is written and reviewed by Prof. Dr Antonio Privitera, consultant colorectal surgeon with fellowship training at Mayo Clinic (USA) and the Royal College of Surgeons (UK), specializing in hemorrhoid diagnosis and minimally invasive treatment.
Frequently Asked Questions
1. Will I need to stay in hospital overnight?
Usually no---hemorrhoidectomy is typically day-case (home the same day). Occasionally we keep patients overnight if:
Significant bleeding risk
Lives alone and has no help at home
Medical conditions requiring observation
2. How bad is the first bowel movement?
It's what patients fear most. Honest answer: it's uncomfortable, but manageable with proper stool softeners. The anticipation is often worse than reality. Each subsequent bowel movement is easier
3. Can I avoid surgery if I'm willing to live with symptoms?
That's a personal decision. Some people with Grade IV live with chronic symptoms because they don't want surgery. But understand: symptoms won't improve on their own and may worsen over time. Surgery is the only definitive treatment.
4. Will hemorrhoids come back after surgery?
Recurrence is 5-10% over 5-10 years. New hemorrhoids can form if you develop chronic constipation or straining again. Maintaining good bowel habits minimizes risk.
5. How long off work?
Desk job: 7-14 days
Physical labor: 14-21 days
Very heavy manual labor: 3-4 weeks
6. When can I resume sex?
Usually 2-3 weeks, or when comfortable. Communicate with your partner and go slowly.
7. Is laser hemorrhoidectomy less painful than traditional?
Evidence is mixed. Some studies show slightly less pain with laser-assisted hemorrhoidectomy; others show no difference. The technique matters less than proper pain management and stool softeners.
8. What if I'm on blood thinners?
You'll need to stop them before surgery (with cardiologist guidance).This is coordinated between your surgeon and cardiologist to balance bleeding risk vs clotting risk.
9. Will I be incontinent after surgery?
Highly unlikely if surgery is performed properly. Temporary urgency or minor seepage can occur during healing but resolves within weeks to months in vast majority of cases.
10. Can I have surgery while pregnant or breastfeeding?
We typically defer elective hemorrhoid surgery until after delivery and breastfeeding. Pregnancy-related hemorrhoids often improve postpartum. If surgery is truly necessary, it can be done during pregnancy but is avoided when possible.
References and Medical Sources
This article is based on current surgical evidence:
1. American Society of Colon and Rectal Surgeons Guidelines – Surgical management of hemorrhoids. Davis BR, Lee-Kong SA, Migaly J, Feingold DL, Steele SR. The American Society of Colon and Rectal Surgeons Clinical Practice Guidelines for the Management of Hemorrhoids. Dis Colon Rectum. 2018;61(3):284-292. PubMed
2. Hemorrhoidectomy Outcomes and Pain Management – Modern approaches to postoperative care. Simillis C, Thoukididou SN, Slesser AA, Rasheed S, Tan E, Tekkis PP. Systematic review and network meta-analysis comparing clinical outcomes and effectiveness of surgical treatments for haemorrhoids. Br J Surg. 2015;102(13):1603-18. PubMed
3. Recurrence Rates After Hemorrhoidectomy – Long-term follow-up studies. Jayaraman S, Colquhoun PH, Malthaner RA. Stapled versus conventional surgery for hemorrhoids. Cochrane Database Syst Rev. 2006;(4):CD005393. PubMed
Medical Review: This content was written and reviewed by Professor training at the Mayo Clinic and Royal College of Surgeons (UK), and European Board Certification in Colorectal Surgery.
Assessment for Grade IV Hemorrhoids: Is Surgery Necessary?
Proper examination determines hemorrhoid grade—then we discuss whether surgery is needed or if less invasive options might work.
📱 WhatsApp: +971 55 318 8469
📞 Phone: +971 55 318 8469
🌐 Book Online:
Dubai Locations:
- Medcare Medical Centre, Discovery Gardens
- Medcare Women and Children Hospital
- Medcare Royal Specialty Hospital
- Clemenceau Medical Centre
- Aster Hospital, Qusais
If surgery is necessary, I’ll explain exactly what to expect—no sugarcoating, but also no unnecessary fear.
Professor Dr. Antonio Privitera
Fellowship Training: Mayo Clinic | Royal College of Surgeons (UK)
European Board Certified in Colorectal Surgery
About the Author
