
Hemorrhoids and travel explained by Prof. Dr Antonio Privitera. Learn how to manage symptoms and travel more comfortably from Dubai. Our hemorrhoid treatment in Dubai explains how early treatment prevents the complications described in this article. treatment, they resolve without serious problems. But complications can occur—and some require urgent medical attention.
I’m Professor Dr. Antonio Privitera, Fellow of the American Society of Colon and Rectal Surgery and Fellow of the Royal College of Surgeons, the only surgeon in the world with both a Mayo Clinic and University of London Colorectal Surgery Fellowship, practicing across Dubai.
Why understanding complications matters:
- Recognize warning signs early
- Know when symptoms require urgent care
- Prevent serious problems through timely treatment
- Understand that most complications are treatable
Common complications:
- Thrombosed hemorrhoids (blood clot)
- Strangulated hemorrhoids (blood supply cut off)
- Severe bleeding causing anemia
- Infection or abscess
- Chronic bleeding leading to iron deficiency
This comprehensive guide covers:
- Types of complications and symptoms
- Emergency vs non-emergency situations
- Treatment for each complication
- Prevention strategies
- Long-term outlook
For urgent hemorrhoid complications:
Experiencing symptoms like these? A discreet same-day specialist assessment is available across Dubai.
WhatsApp: +971 55 318 8469 | Phone: +971 55 318 8469
Medcare Discovery Gardens (Dubai)
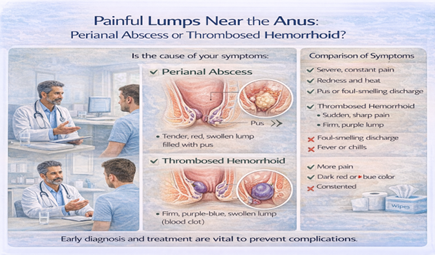
Thrombosed Hemorrhoid: Blood Clot Formation
What Is It:
A blood clot forms inside an external hemorrhoid, causing sudden severe pain and swelling.
How it happens:
- Increased pressure causes blood to clot
- Usually external hemorrhoid (occasionally prolapsed internal)
- Sudden onset—often appears overnight
Symptoms:
Classic presentation:
- Sudden severe pain (within hours)
- Hard, tender lump near anus
- Purple or blue color (clot visible through skin)
- Pain worsens with sitting, walking, bowel movements
- Swelling around anus
Pain pattern:
- Peak pain: First 48-72 hours
- Gradually improves over 2-3 weeks
- Lump may remain for 4-6 weeks as clot reabsorbs
When to Seek Care:
Within 48-72 hours of onset:
- Excision under local anesthesia provides immediate relief
- Simple office procedure (15-20 minutes)
- Pain improves dramatically within hours
- Much better than waiting weeks for natural resolution
After 72 hours:
- Excision less beneficial (clot organizing, harder to remove)
- Usually managed conservatively:
- Ice packs
- Pain medication
- Sitz baths
- Witch hazel
- Time (2-3 weeks to resolve)
Why Treatment Window Matters:
Early excision (within 48-72 hours):
- Clot is fresh, easy to remove
- Immediate pain relief
- Faster overall resolution
Late excision (after 72 hours):
- Clot hardening, more difficult
- Less dramatic pain improvement
- Often not worth surgical intervention at this point
The lesson: Sudden severe anal pain with visible lump = call surgeon immediately.
Strangulated Hemorrhoid: Emergency Situation
What Is It:
An internal hemorrhoid prolapses (comes out) and the anal sphincter
clamps down, cutting off blood supply.
Why it’s serious:
- Tissue without blood supply dies (necrosis)
- Extremely painful
- Risk of infection
- Requires urgent treatment
Symptoms:
Presentation:
- Prolapsed tissue stuck outside that won’t go back in
- Severe constant pain (often worse than thrombosed)
- Purple or black color (indicating dying tissue)
- Swelling progressively worsens
- Possible fever if infection develops
Urgent Treatment Required:
Options:
1. Manual reduction (pushing back in if caught early)
2. Emergency hemorrhoidectomy (if tissue non-viable)
3. Hospital admission for monitoring, IV medications
Delay risks:
- Tissue death
- Infection spreading
- Sepsis (rare but serious)
This is a true emergency—seek immediate care.
Prevention:
Who’s at risk:
- Grade III-IV hemorrhoids
- Chronic straining
- Delaying treatment of prolapsing hemorrhoids
How to prevent:
- Address prolapsing hemorrhoids early
- Don’t strain during bowel movements
- Seek treatment before hemorrhoids reach Grade IV
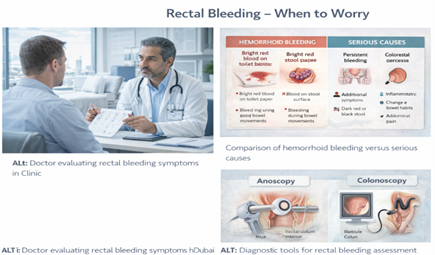
Severe Bleeding and Anemia
Acute Heavy Bleeding:
What constitutes “heavy”:
- Blood dripping continuously into toilet
- Soaking through multiple pads
- Large clots
- Bleeding not stopping after bowel movement
Immediate concerns:
- Rapid blood loss
- Hemodynamic instability (low blood pressure, rapid heart rate)
- Feeling weak, dizzy, faint
This requires emergency evaluation:
- May need blood work to check hemoglobin
- May need intervention to stop bleeding
- Rarely: blood transfusion if severe
Chronic Bleeding Leading to Anemia:
More common scenario:
- Small to moderate bleeding with each bowel movement
- Continues for weeks or months
- Gradual iron deficiency develops
Symptoms of anemia:
- Fatigue, weakness
- Shortness of breath
- Pale skin, pale inner eyelids
- Dizziness, lightheadedness
- Rapid heartbeat
- Cold hands and feet
Diagnosis:
- Blood test (complete blood count)
- Shows low hemoglobin, low iron
- Confirms bleeding as cause
Treatment:
- Stop the bleeding: Treat hemorrhoids definitively
- Replace iron: Oral iron supplements (3-6 months)
- Dietary iron: Red meat, leafy greens, fortified cereals
- Monitor: Repeat blood work to confirm improvement
Prevention:
- Don’t ignore persistent bleeding
- “Just a little blood each time” adds up over months
- Seek treatment before anemia develops
Infection and Abscess
Perianal Abscess:
What is it:
- Pus collection near anus
- Usually not directly from hemorrhoids
- But can occur after hemorrhoid procedures or if strangulated
hemorrhoid becomes infected
Symptoms:
- Severe throbbing pain (constant, worsening)
- Fever (often >38°C)
- Visible swelling, redness near anus
- Warmth to touch
- Sometimes pus drainage
Treatment required:
- Incision and drainage under anesthesia
- Antibiotics for surrounding infection
- Cannot heal on its own—abscess must be drained
Complications if untreated:
- Infection spreading
- Fistula formation (abnormal tunnel from abscess to skin or rectum)
- Sepsis (rare but life-threatening)
Infection After Hemorrhoid Procedures:
Risk factors:
- Poor hygiene during recovery
- Contamination of surgical site (hard to avoid given location)
- Diabetes, immunosuppression
- Smoking
Signs of infection:
- Increasing pain after initial improvement
- Fever
- Pus drainage
- Foul odor
- Redness, warmth spreading
Treatment:
- Antibiotics
- Enhanced hygiene (sitz baths)
- Possible wound care
- Rarely: drainage if abscess forms
Prevention:
- Follow post-operative hygiene instructions
- Sitz baths as directed
- Complete antibiotic course if prescribed
- Report concerning symptoms early
If symptoms persist or are not improving, a specialist assessment in Dubai can help determine the most appropriate treatment.
Portal Vein Thrombosis (Rare but Serious)
What Is It:
Blood clot in the portal vein (carries blood from intestines to liver).
Connection to hemorrhoids:
- Extremely rare complication
- Can occur after aggressive hemorrhoid procedures
- Infection from perianal area spreading to portal circulation
Symptoms:
- Severe abdominal pain
- Fever
- Nausea, vomiting
- Jaundice (yellowing of skin, eyes)
This is a medical emergency requiring immediate hospital care.
How rare:
- Fewer than 100 cases reported worldwide in literature
- Usually in patients with other risk factors (liver disease, clotting disorders)
Prevention:
- Proper surgical technique
- Prompt treatment of infections
- Not a reason to avoid necessary hemorrhoid treatment
Fecal Incontinence (After Surgery)
What Is It:
Inability to control bowel movements or gas.
When it occurs:
- Rare complication of hemorrhoidectomy
- Sphincter muscle damage during surgery
- Over-aggressive sphincterotomy (if done for fissure treatment alongside hemorrhoids)
Types:
- Minor: Occasional gas leakage, difficulty with liquid stool
- Major: Inability to control solid stool (very rare)
Risk factors:
- Prior sphincter damage (childbirth injury, trauma)
- Complex or multiple previous surgeries
- Inexperienced surgeon
Prevention:
- Choose experienced colorectal surgeon
- Proper surgical technique preserving sphincter
- Discuss risk factors with surgeon before procedure
Treatment if it occurs:
- Often improves with time (several months)
- Pelvic floor physical therapy
- Dietary modifications (fiber to bulk stool)
- Medications to slow transit if needed
- Rarely: surgical repair
Anal Stenosis (Narrowing)
What Is It:
Narrowing of anal canal after healing from hemorrhoidectomy.
Causes:
- Excessive tissue removed during surgery
- Scarring during healing
- Chronic inflammation
Symptoms:
- Difficulty passing stool (feels like obstruction)
- Thin, pencil-like stools
- Pain with bowel movements
- Constipation worsening
Prevention:
- Conservative tissue removal during surgery
- Proper surgical technique
- Following post-operative care (sitz baths, dilation exercises if recommended)
Treatment if it occurs:
- Mild: Fiber, stool softeners, gradual dilation
- Moderate: Office-based dilation procedures
- Severe: Surgical correction (anoplasty)
Recurrence as a “Complication”
Is Recurrence a Complication?
Not technically a complication, but a treatment failure or new hemorrhoid formation.
Rates vary by treatment:
- Banding: 10-30% over 5 years
- Laser/THD: 10-20%
- Hemorrhoidectomy: 5-10%
Why recurrence occurs:
- Incomplete initial treatment
- Return to causative habits (constipation, straining)
- New hemorrhoid formation
- Genetic predisposition
Prevention:
- Appropriate initial treatment for grade
- Maintain prevention strategies long-term
- Address underlying causes
Not an emergency, but requires retreatment if symptomatic.
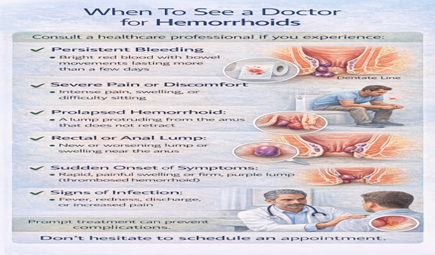
Warning Signs: When to Seek Immediate Care Call Surgeon or Go to Emergency Department If:
🚨 EMERGENCY SIGNS:
Heavy Bleeding:
- Soaking through pads repeatedly
- Blood dripping continuously
- Large clots
- Feeling dizzy, weak, faint
Severe Uncontrolled Pain:
- Pain not relieved by medication
- Sudden onset severe pain (possible thrombosed or strangulated)
- Cannot sit, walk, or function
Fever with Anal Pain:
- Temperature >38°C (100.4°F)
- Chills
- Visible swelling, redness, pus
Strangulated Hemorrhoid:
- Prolapsed tissue won’t go back in
- Purple or black color
- Progressively worsening pain and swelling
Inability to Urinate:
- Cannot pass urine >12 hours
- Associated with severe pain/swelling
Abdominal Pain with Rectal Symptoms:
- Severe abdominal pain
- Nausea, vomiting
- Could indicate rare but serious complication
Call Surgeon Soon (Same Day or Next Day):
Persistent Moderate Symptoms:
- Bleeding continuing despite treatment
- Pain worsening instead of improving
- Signs of infection (increasing redness, warmth, discharge)
- Post-operative concerns
New or Changing Symptoms:
- Symptoms different from your usual pattern
- Uncertainty about severity
Long-Term Outlook After Complications
Most Complications Are Treatable:
Thrombosed hemorrhoid:
- Resolves completely with treatment
- No long-term effects
- Can recur if risk factors continue
Strangulated hemorrhoid:
- Requires surgery but outcome good
- Full recovery expected
- Addresses underlying Grade IV disease
Anemia:
- Reversible with iron supplementation
- Once hemorrhoids treated, no recurrence
Infection:
- Responds to antibiotics and drainage
- Heals without long-term issues in most cases
The key: Early recognition and prompt treatment prevent serious outcomes.
Prevention: Avoiding Complications
Primary Prevention:
Treat hemorrhoids before they progress:
- Grade I-II: Simple office procedures
- Grade III: Laser, THD before becoming Grade IV
- Don’t wait for Grade IV strangulation risk
Maintain good bowel habits:
- High fiber, hydration
- No straining
- Don’t delay bowel movements
Seek care early:
- Small problems are easier to fix
- Don’t ignore persistent symptoms
Secondary Prevention:
After treatment:
- Follow post-operative instructions precisely
- Attend follow-up appointments
- Report concerning symptoms early
- Maintain prevention strategies
Choose experienced surgeon:
- Fellowship-trained colorectal surgeon
- Proper technique reduces complication risk
This article is written and reviewed by Prof. Dr Antonio Privitera, consultant colorectal surgeon with fellowship training at Mayo Clinic (USA) and the Royal College of Surgeons (UK), specializing in hemorrhoid diagnosis and minimally invasive treatment.
Frequently Asked Questions
1. What percentage of hemorrhoid patients develop serious
complications?
Serious complications are rare. Thrombosis occurs in 5-10% of hemorrhoid patients. Strangulation, infection, and severe anemia are much less common (<1-2%). Most hemorrhoids are managed without serious issues.
2. Can hemorrhoids cause death?
Hemorrhoids themselves don’t cause death. Extremely rare complications (severe untreated bleeding leading to shock, or portal vein thrombosis with sepsis) are theoretically life-threatening but exceedingly rare with modern medical care.
3. If I have thrombosed hemorrhoid, will it happen again?
Can recur if you have risk factors (constipation, straining, pregnancy). Maintaining good bowel habits reduces recurrence risk significantly.
4. How do I know if bleeding is “too much”?
Soaking through pads, blood dripping continuously, large clots, or feeling weak/dizzy indicates heavy bleeding requiring evaluation. Small amounts on tissue with bowel movements is common with hemorrhoids.
5. Can I develop sepsis from hemorrhoids?
Extremely rare. Sepsis could theoretically occur from severe untreated perianal infection. This is why fever with anal pain requires prompt medical attention.
6. What if I’m alone when emergency occurs?
Call emergency services if unable to get to hospital yourself. For severe bleeding, severe pain, or fever with confusion/weakness, don’t drive yourself.
7. Will insurance cover emergency hemorrhoid care?
Yes, emergency services are typically covered. Pre-authorization not required for true emergencies.
8. Can complications occur years after hemorrhoid surgery?
Late complications (years later) are very rare. Most complications occur during recovery period (first 2-4 weeks). Late recurrence isn’t acomplication, just new hemorrhoid formation.
9. Should I worry about complications if I choose conservative treatment instead of surgery?
Conservative treatment has minimal complication risk. Thrombosis or strangulation can still occur with untreated hemorrhoids, but these are treatable when they arise.
10. Do complications mean my surgeon made a mistake?
Most complications are inherent risks of the condition or procedure, not errors. Experienced surgeons minimize risk but cannot eliminate it completely. Infection, bleeding, and thrombosis can occur despite perfect technique.
The Bottom Line: Awareness Without Fear
Understanding complications helps you:
- Recognize warning signs
- Seek timely care
- Prevent serious outcomes
But don’t let fear prevent necessary treatment:
- Most hemorrhoids are treated safely
- Complications are manageable
- Delaying treatment carries its own risks
The goal: Educated awareness leading to appropriate action, not anxiety.
References and Medical Sources
1. Hemorrhoid Complications Review – Clinical overview. Lohsiriwat V. Treatment of hemorrhoids: A coloproctologist’s view. World J Gastroenterol. 2015;21(31):9245-52. PubMed
2. Thrombosed External Hemorrhoids – Management guidelines. Greenspon J, Williams SB, Young HA, Orkin BA. Thrombosed external hemorrhoids: outcome after conservative or surgical management. Dis Colon Rectum. 2004;47(9):1493-8. PubMed
3. Surgical Complications – Risk factors and outcomes. Simillis C, Thoukididou SN, Slesser AA, Rasheed S, Tan E, Tekkis PP. Systematic review and network meta-analysis comparing clinical outcomes and effectiveness of surgical treatments for haemorrhoids. Br J Surg. 2015;102(13):1603-18. PubMed
Medical Review: This content was written and reviewed by Professor Dr. Antonio Privitera, Fellow of the American Society of Colon and Rectal Surgery and Fellow of the Royal College of Surgeons, the only Colorectal Surgery Fellowship.
Expert Care for Hemorrhoid Complications
Fellowship-trained expertise in managing complex hemorrhoid complications.
Experiencing symptoms like these? A discreet same-day specialist assessment is available across Dubai.
WhatsApp: +971 55 318 8469 | Phone: +971 55 318 8469
Medcare Discovery Gardens (Dubai)
Dubai Locations
- Medcare Medical Centre, Discovery Gardens
- Medcare Women and Children Hospital
- Medcare Royal Specialty Hospital
- Clemenceau Medical Centre
- Aster Hospital, Qusais
About the Author
