
Hemorrhoid treatment in Dubai requires accurate diagnosis and choosing the right technique for your specific condition. Most patients can be treated effectively with modern, minimally invasive procedures when managed by a specialist. I'm Professor Dr. Antonio Privitera, a consultant colorectal surgeon with fellowship training at the Mayo Clinic and in London, and European Board Certification in Colorectal Surgery. I specialize in the diagnosis and treatment of hemorrhoids and other anorectal conditions.
In my practice, I see patients every day who've delayed seeking care because of embarrassment or fear of surgery. The truth is straightforward: most hemorrhoids don't require surgery, and when they do, modern techniques have dramatically reduced pain and recovery time.
What matters most is accurate diagnosis because not all rectal bleeding or discomfort is caused by hemorrhoids and choosing treatment based on the grade and type of hemorrhoid you have, not marketing claims.
Professor Dr. Antonio Privitera Mayo Clinic & University of London Fellowship | FRCS | FASCRS
Discreet same-day assessment available. No referral required.
Medcare Discovery Gardens, Dubai
Here's what sets our approach apart:
- Accurate diagnosis first: We examine you properly (visual inspection, digital exam, anoscopy when needed) to confirm hemorrhoids and rule out other causes.
- Grade-based treatment: We match the treatment to your condition, not the other way around.
- Discreet, same-day assessment available: Privacy matters. We offer complete confidentiality across Dubai.
This guide explains everything you need to know about hemorrhoids, from symptoms and diagnosis to the full range of treatment options available in the UAE.
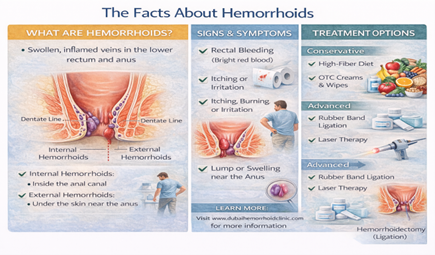
What Are Hemorrhoids?
Hemorrhoids (also called piles) are swollen blood vessels in the lower rectum and anal canal. Everyone has hemorrhoidal tissue these vascular cushions help with continence and sensation. Hemorrhoids become a problem when they enlarge, bleed, prolapse (come out of the anus), or cause pain.
There are two types:
- Internal hemorrhoids: Sit inside the rectum, above the dentate line. They typically don't hurt because they have no pain receptors they primarily bleed.
- External hemorrhoids: Are under the skin around the anus. These can be painful, especially if a clot forms (thrombosed external hemorrhoid).
Symptoms of Hemorrhoids: What You Might Notice
Hemorrhoid symptoms vary depending on whether they're internal or external. Typical experiences include:
- Bleeding: Bright red blood on toilet paper or in the bowl.
- A lump or swelling: A soft lump near the anus or a painful thrombosed clot.
- Itching or irritation: Caused by mucus discharge.
- Discomfort or pain: Especially with external or strangulated hemorrhoids.
Red Flags: Urgent Evaluation Needed
Seek medical care quickly if you experience: Heavy bleeding, dizziness, severe constant pain, fever with swelling, or unexplained weight loss.
Internal vs External Hemorrhoids: Why the Difference Matters
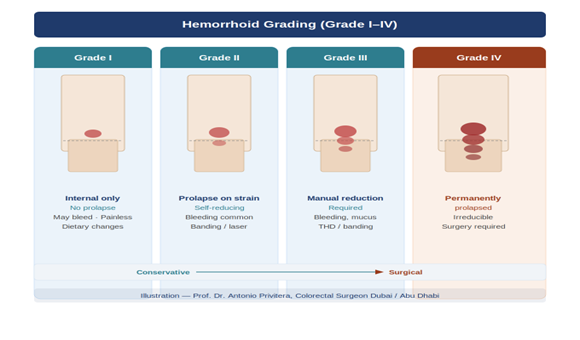
Hemorrhoid Grading System
Grade I: Bleed but don't prolapse.
Grade II: Prolapse during straining but go back in on their own.
Grade III: Prolapse and require manual reduction (pushing back in).
Grade IV: Permanently prolapsed and cannot be pushed back inside.
Why grading matters: Different treatments work for different grades. A Grade IV usually requires surgery, while Grade I often responds to lifestyle changes. The safest approach is grade-based treatment selection.
What Causes Hemorrhoids? (And Dubai-Specific Risk Factors)
Hemorrhoids develop when there's increased pressure on the blood vessels in the rectum and anus. Common causes include:
- Straining during bowel movements: Chronic constipation and hard stools are the most common culprits.
- Prolonged sitting: Especially on the toilet. In Dubai, I see this frequently in office workers who sit 10 to12 hours a day.
- Low-fiber diet: Many expatriates in the UAE eat less fiber than in their home countries.
- Dehydration: Dubai's heat and air conditioning lead to harder stools. Aim for 2.5 to 3 liters of water daily.
- Pregnancy and childbirth: Increased pressure on pelvic veins and hormonal changes.
In my practice, I see patterns: long office hours, dehydration from coffee/tea, eating out frequently (low fiber), and delayed care due to busy schedules.
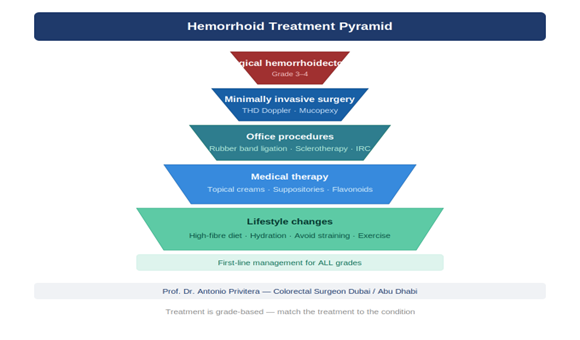
Treatment Options in Dubai: From Conservative Care to Surgery
Treatment depends on the type and grade of hemorrhoid. Here is my approach, from least invasive to most invasive.
Conservative Treatment (First-Line)
For Grade I and early Grade II, lifestyle changes are often all you need. This includes a fiber target of 25 to 35 grams daily and proper hydration.
Office Procedures (Grade I–II)
I place a small band around the base of an internal hemorrhoid. It shrinks and falls off within a week. Best for Grade I and II.
Sclerotherapy & Infrared Coagulation:Chemical injections or light energy to shrink early-grade hemorrhoids.
Minimally Invasive Operating Room Procedures
Laser fiber shrinks the hemorrhoid from inside. Recovery is 3 to 7 days. Ideal for Grade II and III.
THD (Transanal Hemorrhoidal Dearterialization):Using Doppler ultrasound to tie off arteries. No tissue is cut, meaning less pain and 5 to10 days recovery.
Surgical Treatment: Hemorrhoidectomy
For Grade 4 hemorrhoids or large mixed cases, surgical removal is the most definitive cure with the lowest recurrence rate.
Recovery & What to Expect
Recovery depends on the treatment: Office procedures require 1 to 2 days, while hemorrhoid recovery takes 7 to14 days for desk work.
First Visit: We perform a visual inspection, digital rectal exam, and anoscopy. If there are red flags, I may recommend a colonoscopy to rule out other issues.
My Approach: What Sets This Practice Apart
I believe in matching the treatment to your specific situation. If you were my family member, I'd tell you: don't be embarrassed, get a proper exam, and don't rush into expensive surgery if a simpler procedure works.
I check for skin tags indicating a previous thrombosed hemorrhoid emergency and look for the whole picture, ensuring you get a grade-based plan that fits your Dubai lifestyle.
About the Author
