
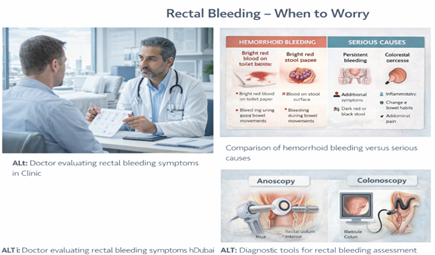
How We Diagnose the Cause of Your Bleeding
Hemorrhoid bleeding in Dubai should never be ignored because rectal bleeding can have different causes. Early specialist assessment helps confirm the diagnosis and identify when urgent investigation is needed. A complete guide to all diagnosis and treatment options is available in our hemorrhoid treatment in Dubai.
your assessment:
Step 1: Detailed History
I’ll ask about:
- When bleeding started and how often it occurs
- What the bleeding looks like (color, amount, pattern)
- Associated symptoms (pain, itching, prolapse, change in bowel habits, weight loss)
- Bowel habits (constipation, diarrhea, straining)
- Your age and whether you’ve had colon screening
- Family history of colorectal cancer, polyps, or inflammatory bowel disease
- Medical history (previous bleeding, hemorrhoids, other conditions)
- Medications (blood thinners, aspirin, NSAIDs can increase bleeding)
Step 2: Physical Examination
A proper diagnosis requires examination. This includes:
Experiencing symptoms like these? A discreet same-day specialist assessment is available across Dubai.
WhatsApp: +971 55 318 8469 | Phone: +971 55 318 8469
Medcare Discovery Gardens (Dubai)
Visual Inspection
Looking at the perianal area (around the anus) to identify:
- External hemorrhoids
- Skin tags (from previous hemorrhoids)
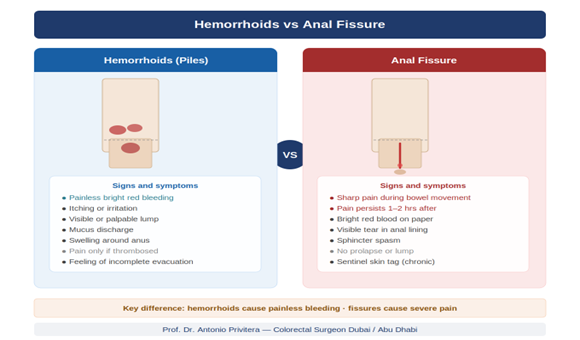
- Anal fissures (tears causing bleeding)
- Signs of infection or abscess
- Visible prolapsing internal hemorrhoids
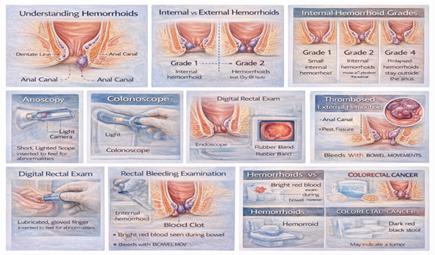
Digital Rectal Exam (DRE)
Inserting a gloved, lubricated finger into the rectum to:
- Feel for masses or polyps within reach (lower rectum)
- Assess sphincter tone
- Check for tenderness or abnormalities
- Test stool for blood (fecal occult blood test)
This takes about 30 seconds and is mildly uncomfortable but not painful.
Anoscopy
Using a small, lighted scope (anoscope) inserted a few centimeters into the anus to:
- Directly visualize internal hemorrhoids (the most common cause of bleeding)
- See if hemorrhoids are actively bleeding
- Identify fissures, ulcers, or other sources of bleeding
- Assess hemorrhoid grade (I-IV)
Anoscopy takes 1-2 minutes and provides the clearest view of internal hemorrhoids. You’ll feel pressure but it’s not painful.
Step 3: Deciding on Further Testing
Based on examination findings, your age, and red flags, I’ll determine if you need:
Colonoscopy (Full Colon Examination)
Who needs it:
- Anyone 40 or older with rectal bleeding (if never screened or not screened recently)
- Patients with red flag symptoms (weight loss, change in bowel habits, family history, anemia)
- Bleeding that doesn’t clearly match hemorrhoids on examination
- Persistent bleeding despite treatment for hemorrhoids
What it involves:
A flexible scope examines the entire colon while you’re under sedation.
This allows us to:
- Identify and remove polyps
- Diagnose colorectal cancer at early, curable stages
- Diagnose inflammatory bowel disease (Crohn’s, ulcerative colitis)
- Rule out other causes of bleeding
Preparation:
You’ll need bowel preparation (drinking a cleansing solution the day before). The procedure itself takes 20-30 minutes, and you’ll go home the same day.
Flexible Sigmoidoscopy (Lower Colon Only)
Examines the lower third of the colon (rectum and sigmoid colon). Less preparation needed than colonoscopy, but only examines part of the colon. Used less commonly now—if we’re doing a scope, we usually examine the entire colon (colonoscopy).
When Colonoscopy Can Wait
If you’re under 40, have no red flags, examination clearly shows bleeding hemorrhoids, and you have no family history of colon cancer, we may treat the hemorrhoids first and reserve colonoscopy for if bleeding persists or other symptoms develop.
But: This decision is made after proper examination, not based on symptoms alone
Who Needs Colonoscopy? UAE Screening Guidelines
Clear Indications for Colonoscopy:
Age 40+ (UAE Guideline)
In the UAE, colorectal cancer screening typically begins at age 40 for average-risk individuals. If you’re 40 or older with rectal bleeding, colonoscopy is recommended even if hemorrhoids are present. Department of Health and Cleveland Clinic.
Family History of Colorectal Cancer or Polyps
If a first-degree relative (parent, sibling, child) had colorectal cancer or advanced polyps, screening should start 10 years earlier than the age at which your relative was diagnosed, or at age 40, whichever is earlier.
Example: If your father had colon cancer at age 50, you should start screening at age 40.
Personal History of Polyps or Inflammatory Bowel Disease
If you’ve had polyps removed previously or have Crohn’s disease or ulcerative colitis, you need regular surveillance colonoscopy regardless of age.
Any Red Flag Symptoms
Regardless of age:
- Unintentional weight loss
- Change in bowel habits lasting more than 2 weeks
- Blood mixed throughout stool (not just on surface)
- Anemia (low blood counts)
- Family history of hereditary colon cancer syndromes
When We Can Defer Colonoscopy:
If you’re under 40, have no family history, examination shows clear hemorrhoid bleeding, and you have no red flags, we may:
1. Treat the hemorrhoids first
2. Monitor response
3. Recommend colonoscopy if bleeding persists despite treatment or if symptoms change
This approach is individualized and discussed with each patient.
If symptoms persist or are not improving, a specialist assessment in Dubai can help determine the most appropriate treatment.
What to Expect at Your Diagnostic Appointment
Before Your Visit:
What to bring:
- List of medications (especially blood thinners, aspirin, NSAIDs)
- Details about bleeding (when it started, how often, what triggers
- Family medical history
- Previous test results if available (colonoscopy reports, blood tests)
Preparation:
- No special preparation needed for examination (you don’t need an enema or fasting)
- Wear comfortable clothing
- If you’re very anxious, it may help to take a friend or family member During the Visit (Usually 20-30 Minutes):
1. Discussion (10-15 minutes): I’ll review your symptoms, history, and concerns
2. Examination (5-10 minutes): Visual inspection, digital exam, anoscopy
3. Discussion of findings (5-10 minutes): I’ll explain what I found and recommend next steps
Possible Outcomes:
Outcome 1: Clear Hemorrhoid Bleeding (Low Risk)
- Age under 40, no red flags, examination shows bleeding hemorrhoids
- Plan: Treat hemorrhoids (dietary changes, office procedure if needed), monitor response
- Follow-up: Return if bleeding persists or symptoms change
Outcome 2: Hemorrhoids Present, But Colonoscopy Needed
Age 40+, or red flags present, or never had screening Plan: Treat hemorrhoids + schedule colonoscopy to examine full colon
- Why both: We need to confirm there’s nothing else causing bleeding
Outcome 3: Examination Doesn’t Clearly Show Hemorrhoids
Source of bleeding unclear, or findings don’t match symptoms
- Plan: Colonoscopy to identify cause
Outcome 4: Red Flags Present
- Urgent colonoscopy (within 1-2 weeks)
- Blood tests (complete blood count to check for anemia)
- Possible CT scan if concerning findings
If Colonoscopy Is Recommended:
- We’ll explain why it’s needed and what we’re looking for
- You’ll receive bowel preparation instructions
- The procedure is scheduled (usually within 1-4 weeks depending on urgency)
- You’ll need someone to drive you home after (due to sedation)
My Approach: Why I Always Examine Before Concluding “It’s Just Hemorrhoids”
In my years of training across the United States, United Kingdom, and now the UAE, I’ve learned an important lesson: Most rectal bleeding is from hemorrhoids. But assuming all rectal bleeding is hemorrhoids without examination can be dangerous.
Here’s a real scenario I see regularly in my Dubai practice: A 45-year-old professional comes in with bleeding. He’s been told by his GP (over the phone or based on symptoms alone) that he has hemorrhoids. He’s been using creams for 3 months. Bleeding continues. When I examine him, I find small hemorrhoids—but also feel a mass on digital rectal exam. Colonoscopy reveals a rectal cancer that’s still curable because we caught it relatively early.
Did he have hemorrhoids? Yes. Was that the only problem? No.
This is why I insist on examination before concluding the diagnosis. And this is why, in the UAE where colorectal cancer screening starts at 40, any bleeding in patients 40+ prompts me to recommend colonoscopy even when hemorrhoids are obvious.
Another pattern I see in Dubai: Patients delay seeking care because of embarrassment or busy work schedules. By the time they come in, bleeding has been present for months or even years. If you’re 40+, those months or years matter—a polyp can become cancer, an early cancer can become advanced.
Don’t let embarrassment delay diagnosis. I see this every single day.
Your symptoms aren’t unusual or shocking to me.
This article is written and reviewed by Prof. Dr Antonio Privitera, consultant colorectal surgeon with fellowship training at Mayo Clinic (USA) and the Royal College of Surgeons (UK), specializing in hemorrhoid diagnosis and minimally invasive treatment.
FAQS
1. Can I just assume it’s hemorrhoids if the blood is bright red?
Bright red blood is typical of hemorrhoids, but it’s not exclusive to hemorrhoids. Anal fissures, rectal polyps, and even rectal cancer can cause bright red bleeding. The only way to know for sure is examination.
2. I have hemorrhoids that I can feel. Does that mean the bleeding is definitely from them?
Not necessarily. Hemorrhoids (internal or external) and colon polyps can coexist. The presence of hemorrhoids doesn’t rule out other causes of bleeding. If you’re 40+ or have red flags, you need colonoscopy even if hemorrhoids are present.
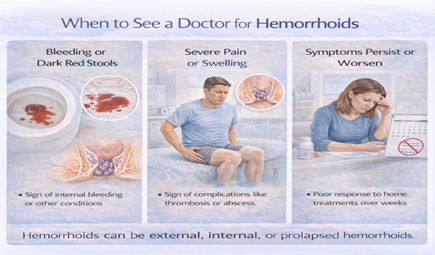
3. How much bleeding is normal with hemorrhoids?
Hemorrhoid bleeding varies from streaks on toilet paper to several tablespoons in the toilet bowl. Most hemorrhoid bleeding stops on its own within minutes after a bowel movement. If you’re soaking through toilet paper repeatedly, bleeding continues for more than 10-15 minutes, or you’re filling the toilet bowl with blood, seek immediate care.
4. I’m 35 with no family history. Do I really need a colonoscopy?
If examination clearly shows bleeding hemorrhoids, you have no red flags, and you’re under 40 with no family history, we can often treat the hemorrhoids first and monitor. If bleeding persists despite treatment, or if any red flags develop, colonoscopy is recommended.
5. I’m 42 but I had a colonoscopy 2 years ago that was normal. Do I
need another one?
If your recent colonoscopy was normal (no polyps) and you have clear hemorrhoid bleeding on examination, you probably don’t need immediate repeat colonoscopy. However, if bleeding doesn’t improve with hemorrhoid treatment, or if you develop new symptoms, repeat colonoscopy may be indicated.
6. Will colonoscopy hurt?
No. You’ll be under sedation (conscious sedation or deep sedation depending on the facility). Most patients remember nothing about the procedure. You’ll have mild bloating or cramping afterward from air used during the scope, but this resolves quickly.
7. How accurate is anoscopy? Can it miss things?
Anoscopy is excellent for visualizing the anal canal and lower rectum (where internal hemorrhoids are). It can see bleeding hemorrhoids, fissures, and low rectal problems. However, it only examines the first few centimeters—it can’t see the rest of the colon. This is why colonoscopy is needed for complete evaluation.
8. Can I do a stool test instead of colonoscopy?
Fecal occult blood tests (FOBT) or fecal immunochemical tests (FIT) can detect hidden blood in stool and are used for screening in asymptomaticpeople. However, if you’re already having visible bleeding, these tests don’t add useful information—you already know there’s blood. Colonoscopy is the gold standard for evaluation of visible bleeding.
9. What if I’m too embarrassed to have an examination?
I understand this concern, and it’s common. Here’s what I tell patients: I see this every single day. Your anatomy is not unusual, your symptoms aren’t shocking, and there’s nothing to be embarrassed about. The examination takes a few minutes, and the information it provides can be lifesaving. Embarrassment should never be a barrier to getting proper care.
10. How long does bleeding from hemorrhoids last?
With treatment (dietary changes, fiber, hydration, possibly office procedures like rubber band ligation), hemorrhoid bleeding usually improves within 1-4 weeks. If bleeding persists beyond 4-6 weeks despite treatment, further evaluation (colonoscopy) is recommended to rule out other causes.
Next Steps: Getting Properly Diagnosed
If you’re experiencing rectal bleeding:
Step 1: Get Examined
Don’t assume it’s hemorrhoids based on symptoms alone. Proper examination (visual inspection, digital rectal exam, anoscopy) confirms the diagnosis.
Step 2: Determine If You Need Colonoscopy
Based on your age, risk factors, and examination findings, we’ll discuss whether colonoscopy is recommended.
Step 3: Treat the Cause
If hemorrhoids: Conservative treatment or office procedures
If fissure: Medical management or minor procedure
If colonoscopy shows polyps: Remove them (prevents cancer)
If cancer: Early detection means high cure rates
The sooner you get diagnosed, the simpler treatment tends to be.
References and Medical Sources
This article is based on current medical evidence and clinical guidelines:
1. UAE Colorectal Cancer Screening Guidelines – Abu Dhabi Department of Health recommends screening starting at age 40. Abu Dhabi Public Health Center.
2. Cleveland Clinic Abu Dhabi Screening Guidelines – Local protocols for colorectal cancer screening. CCAD Guidelines
3. American Society of Colon and Rectal Surgeons Guidelines – Evaluation and management of hemorrhoids and rectal bleeding. Davis BR, Lee-Kong SA, Migaly J, Feingold DL, Steele SR. The American Society of Colon and Rectal Surgeons Clinical Practice Guidelines for the Management of Hemorrhoids. Dis Colon Rectum. 2018;61(3):284-292. PubMed.
4. Colorectal Cancer Screening Guidelines – International consensus on screening ages and risk factors. Rex DK, Boland CR, Dominitz JA, et al. Colorectal Cancer Screening: Recommendations for Physicians and Patients from the U.S. Multi-Society Task Force on Colorectal Cancer. Am J Gastroenterol. 2017;112(7):1016-1030. PubMed.
Medical Review: This content was written and reviewed by Professor training at the Mayo Clinic and Royal College of Surgeons (UK), and
European Board Certification in Colorectal Surgery.
Schedule Your Diagnostic Assessment
Don’t assume bleeding is “just hemorrhoids” without proper examination—especially if you’re 40 or older.
📱 WhatsApp: +971 55 318 8469
📞 Phone: +971 55 318 8469
🌐 Book Online:
Dubai Locations:
- Medcare Medical Centre, Discovery Gardens
- Medcare Women and Children Hospital
- Medcare Royal Specialty Hospital
- Clemenceau Medical Centre
- Aster Hospital, Qusais
Same-day appointments available for evaluation. All consultations are private and confidential.
Professor Dr. Antonio Privitera
Fellowship Training: Mayo Clinic | Royal College of Surgeons (UK) European Board Certified in Colorectal Surgery
About the Author
