
THD hemorrhoid treatment in Dubai is a minimally invasive procedure that can be highly effective for selected internal hemorrhoids while reducing postoperative pain compared with traditional excision. Proper patient selection is essential for the best outcome.
- HAL: Hemorrhoidal Artery Ligation
- RAR: Recto-Anal Repair (also called mucopexy)
The Concept:
Traditional surgery (hemorrhoidectomy):
- Cuts away hemorrhoid tissue
- Leaves wounds that take weeks to heal Painful recovery
THD approach:
- Addresses the ROOT CAUSE: excessive blood flow to hemorrhoids
- Cuts off blood supply → hemorrhoids shrink
- Repositions prolapsed tissue
- No tissue removed → faster healing, less pain
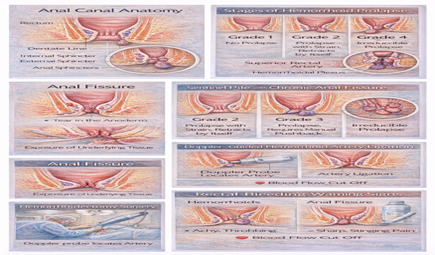
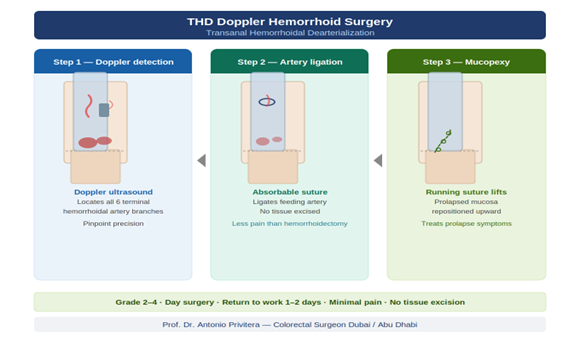
How THD Works: The Two-Step Process
Step 1: HAL (Hemorrhoidal Artery Ligation)
What happens:
1. Special proctoscope with built-in Doppler ultrasound is inserted into rectum
2. Doppler detects arterial blood flow (makes audible signal when artery is located)
3. I identify 4-6 hemorrhoidal arteries feeding blood to hemorrhoids (usually 6 main arteries around the circumference)
4. Each artery is ligated (tied off) with absorbable sutures through the rectal mucosa
5. Blood supply to hemorrhoids is cut off
Result: Without blood supply, hemorrhoid tissue shrinks over following weeks.
Step 2: RAR (Recto-Anal Repair / Mucopexy)
What happens:
1. Prolapsed hemorrhoidal tissue is identified
2. Tissue is lifted back up to its normal anatomical position
3. Stitched to the rectal wall with absorbable sutures
4. Multiple plications (folds) are created to reposition all prolapsed tissue
Result: Prolapse is corrected, tissue stays in proper position.
The Complete Procedure:
Duration: 45-60 minutes
Anesthesia: Spinal or general anesthesia
Hospital stay: Usually day-case (home same day) or overnight
What you won’t feel: Pain during procedure (you’re anesthetized)
What’s different from hemorrhoidectomy:
- No tissue cut away
- No open wounds
- Stitches are internal (you don’t see them)
- Stitches dissolve on their own over 2-4 weeks
Who Benefits Most from THD?
Ideal Candidates:
Grade II-III Internal Hemorrhoids:
- THD works best for these grades
- Studies show 80-90% success for Grade II-III
Failed Conservative Treatment:
- Tried fiber, hydration, lifestyle changes
- Symptoms persist
Failed or Unsuitable for Banding:
- Hemorrhoids too large for effective banding
- Banding was tried but symptoms returned
Want to Avoid Hemorrhoidectomy:
- THD offers middle ground: more definitive than banding, less invasive than surgery
Minimal External Component:
- THD addresses internal hemorrhoids
- If large external hemorrhoids present, may need additional treatment or hemorrhoidectomy instead
Not Ideal Candidates:
Grade I Hemorrhoids:
- Too early for THD
- Banding is simpler, equally effective
Grade IV with Large External Component:
- THD won’t address external tissue For these Grade 4 hemorrhoids in Dubai or severe cases
- Hemorrhoidectomy usually better option
Significant Skin Tags:
- THD doesn’t remove skin tags
- May need separate excision
Recovery Timeline: What to Actually Expect
Day of Procedure:
- Procedure in morning usually
- Recovery room 1-2 hours
- Discharged same day (or stay overnight if preferred)
- Pain medication, stool softeners, instructions provided
Pain level: 2-4/10 (medications on board)
Days 1-3:
Pain level: 4-6/10 (managed with oral pain medication)
What you’ll feel:
- Moderate discomfort in rectal area
- Feeling of fullness or pressure
- Anxiety about first bowel movement (day 2-3 typically)
First bowel movement:
- Will be uncomfortable but manageable with stool softeners
- Less painful than after hemorrhoidectomy
- Takes stool softener night before, morning of
Activities:
- Rest at home
- Short walks encouraged
- Sitz baths 3-4 times daily
Days 4-7:
Pain level: 3-5/10
Improvement:
- Each day noticeably better than previous
- Bowel movements less uncomfortable
- Can do light activities around home
Most patients: Still off work this week
Week 2:
Pain level: 2-3/10
Activities:
- Many return to desk work end of week 1 or during week 2
- Can walk 20-30 minutes comfortably
- Still avoiding heavy lifting, strenuous activity
Week 3-4:
Pain level: 1-2/10
Activities:
- Most back to normal daily activities
- Can resume light exercise (walking, swimming, light weights)
- Still avoiding very heavy lifting
Week 6-8:
Pain level: 0-1/10
Full recovery:
- All activities unrestricted
- Hemorrhoids have shrunk to maximum extent
- Follow-up appointment with surgeon to confirm healing
Success Rates and Long-Term Outcomes
Clinical Evidence:
Success rates (symptom improvement):
- Grade II hemorrhoids: 85-95% success
- Grade III hemorrhoids: 75-85% success
- Grade IV: Variable (depends on external component)
Recurrence rates:
- 10-15% experience some symptom recurrence over 3-5 years
- Lower recurrence than banding
- Higher recurrence than hemorrhoidectomy (but THD is less invasive)
Patient satisfaction:
- Most studies report 80-90% patient satisfaction
- Especially valued: less pain than hemorrhoidectomy, good outcomes
Factors Affecting Success:
Better outcomes:
- Grade II-III internal hemorrhoids (ideal candidates)
- Minimal external component
- Good bowel habits maintained post-procedure (fiber, hydration, no straining)
Poorer outcomes:
- Grade IV with large external component
- Chronic constipation not addressed
- Unrealistic expectations (expecting 100% guarantee)
Reference: Ratto C, Giordano P, Donisi L, et al. Transanal haemorrhoidal dearterialisation (THD) for haemorrhoidal disease: a single-centre study on 1000 consecutive cases. Colorectal Dis. 2017;19(8):750-756. PubMed
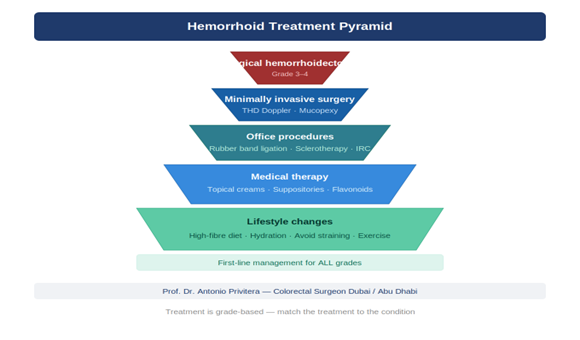
THD vs Other Treatments: When to Choose What
THD vs Rubber Band Ligation:
If symptoms persist or are not improving, a specialist assessment in Dubai can help determine the most appropriate treatment.
Feature Banding THD
Best for Grade I-II Grade II-III
Setting Office Operating room
Anesthesia None Spinal/general
Sessions Often 2-3 One
Recovery 1-2 days 5-10 days
Success (Grade II) Similar Similar
Success (Grade III) Lower Higher
Cost Lower Higher
When to choose banding: Grade I-II, want simplest option, willing todo multiple sessions
When to choose THD: Grade III, banding failed, want single-session
definitive treatment
THD vs Laser Hemorrhoidoplasty:
Feature Laser THD
Mechanism Shrinks tissue with Ligates arteries + energy repositions
Recovery 3-7 days 5-10 days
Success (Grade Good Better III)
Recurrence Moderate Lower
Cost Similar Similar
When to choose laser: Prefer slightly faster recovery, Grade II-III internal only
When to choose THD: Want best long-term results for Grade III, willing to accept slightly longer recovery
THD vs Hemorrhoidectomy:
Feature THD Hemorrhoidectomy
Invasiveness Moderate High
Tissue removed No Yes
Recovery 2-3 weeks 4-6 weeks
Pain Moderate Severe week 1
Treats external No Yes
Recurrence 10-15% 5-10%
When to choose THD: Grade II-III, want to avoid full surgery, minimal external component
When to choose hemorrhoidectomy: Grade IV, large external component, want most definitive treatment
Cost of THD in Dubai
Approximate Costs:
THD procedure: AED 18,000 – 30,000
Included:
- Surgeon fee
- Anesthesiologist
- Operating room facility
- Specialized THD equipment (Doppler proctoscope)
- Post-operative follow-up visits
Not included:
- Pre-operative tests (blood work, ECG if needed)
- Medications (usually AED 200-500)
Insurance Coverage:
Most UAE insurance plans:
- Cover THD for Grade III hemorrhoids (medically necessary)
- May require pre-authorization
- Coverage for Grade II varies (some insurers want banding tried first)
Check with your insurer BEFORE booking procedure.
Payment Options:
Most facilities offer:
- Direct billing to insurance (if covered)
- Payment plans (if self-pay)
- Credit card payment
What Makes a Good THD Surgeon?
Look for:
1. Colorectal Surgery Training:
- Fellowship-trained colorectal surgeon (not just general surgeon)
- Specific training in THD technique
2. Experience:
- Has performed THD regularly (not just once or twice)
- Can discuss success rates and complications honestly
3. Uses Doppler Technology:
- THD requires specialized equipment
- Doppler-guided ligation is more accurate than blind ligation
4. Performs Multiple Procedures:
- Doesn’t only offer THD
- Can recommend banding, laser, or surgery when those are better options
- This indicates they’re choosing treatment based on YOUR anatomy, not their equipment
5. Realistic About Outcomes:
- Explains when THD works well (Grade II-III)
- Explains when other options are better (Grade I or Grade IV)
- Discusses potential for recurrence honestly
Preparing for THD Procedure
Pre-Operative:
1-2 Weeks Before:
- Pre-operative consultation
- Medical clearance (blood tests, ECG if needed)
- Insurance authorization if applicable
Day Before:
- Light diet
- No bowel preparation usually required (unlike colonoscopy)
- Fasting from midnight
Day Of:
- Arrive 1-2 hours before procedure
- Change into gown
- IV line placed
- Meet anesthesiologist
Post-Operative Instructions:
Medications:
- Pain medication (oral)
- Stool softener (ESSENTIAL—start day of procedure)
- Possibly antibiotics (depending on surgeon preference)
Activities:
- Rest day of procedure
- Short walks starting day 1
- Sitz baths 3-4 times daily
- No heavy lifting 2-3 weeks
Diet:
- High fiber starting immediately
- Adequate hydration (2.5-3 liters daily)
Follow-up:
- Usually 1-2 weeks post-procedure
- Surgeon checks healing, addresses concerns
This article is written and reviewed by Prof. Dr Antonio Privitera, consultant colorectal surgeon with fellowship training at Mayo Clinic (USA) and the Royal College of Surgeons (UK), specializing in hemorrhoid diagnosis and minimally invasive treatment.
Frequently Asked Questions
1. Is THD painful?
Less painful than hemorrhoidectomy but not painless. Expect moderate discomfort for first week, managed with oral pain medication. Most patients rate recovery as “uncomfortable but manageable.”
2. Will I need to stay in hospital overnight?
Usually no—THD is typically day-case procedure. Occasionally overnight stay if patient prefers or lives far from hospital.
3. Can THD treat external hemorrhoids?
No. THD addresses internal hemorrhoids. If you have large external hemorrhoids or skin tags, they won’t be treated by THD. May need separate excision or hemorrhoidectomy instead.
4. How long do THD results last?
Studies show good long-term results with 10-15% recurrence over 3-5 years. Maintaining good bowel habits (fiber, hydration, no straining) reduces recurrence risk.
5. What if THD doesn’t work?
If symptoms persist or recur, options include: repeat THD (less common), hemorrhoidectomy (more definitive). Most patients have good outcomes with first THD.
6. Can I have THD if I’ve had previous hemorrhoid treatment?
Usually yes. Previous banding doesn’t preclude THD. Previous hemorrhoidectomy makes THD more complex but possible in some cases.
7. How soon can I return to work?
Desk job: 5-10 days. Physical labor: 10-14 days. Heavy manual work: 14-21 days.
8. Will hemorrhoids come back after THD?
Some patients experience recurrence (10-15% over several years). Lower recurrence than banding, higher than hemorrhoidectomy. Maintaining good bowel habits is key.
9. Is THD available in Dubai?
Yes. Available at major hospitals and specialized colorectal surgery practices. Requires specialized equipment and training, so not all facilities offer it.
10. Should I choose THD or hemorrhoidectomy?
Depends on your grade and external component. Grade II-III with minimal external → THD is excellent option. Grade IV or large external → hemorrhoidectomy usually better. Discuss with surgeon.
References and Medical Sources
THD outcomes based on clinical evidence:
1. Large THD Outcomes Study – Long-term results. Ratto C, Giordano P, Donisi L, et al. Transanal haemorrhoidal dearterialisation (THD) for haemorrhoidal disease: a single-centre study on 1000 consecutive cases. Colorectal Dis. 2017;19(8):750-756. PubMed
2. THD vs Hemorrhoidectomy Comparison – Randomized trial. Denoya PI, Fakhoury M, Chang K, et al. Dearterialization with mucopexy versus haemorrhoidectomy for grade III or IV haemorrhoids: short-term results of a double-blind randomized controlled trial. Colorectal Dis. 2013;15(10):1281-8. PubMed
3. American Society of Colon and Rectal Surgeons Guidelines – Treatment recommendations including THD. Davis BR, Lee-Kong SA, Migaly J, Feingold DL, Steele SR. The American Society of Colon and Rectal Surgeons Clinical Practice Guidelines for the Management of Hemorrhoids. Dis Colon Rectum. 2018;61(3):284-292. PubMed
Medical Review: This content was written and reviewed by Professor training at the Mayo Clinic and Royal College of Surgeons (UK), and European Board Certification in Colorectal Surgery.
THD Assessment in Dubai
I perform THD along with banding, laser, and hemorrhoidectomy—so I recommend based on your anatomy, not my equipment.
Experiencing symptoms like these? A discreet same-day specialist assessment is available across Dubai .
WhatsApp: +971 55 318 8469 | Phone: +971 55 318 8469
Medcare Discovery Gardens (Dubai)
Dubai Locations
Multiple locations with THD capability
Proper examination determines if THD is right for you.
Professor Dr. Antonio Privitera
Fellowship Training: Mayo Clinic | Royal College of Surgeons (UK)
About the Author
