
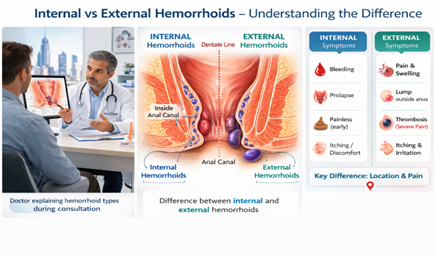
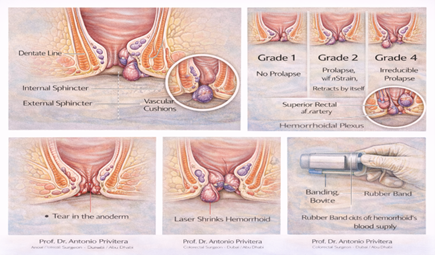
What Is the Dentate Line?
Internal and external hemorrhoids in Dubai cause different symptoms and often require different treatment approaches. Understanding the difference is essential for accurate diagnosis and effective care. Our complete hemorrhoid treatment in Dubai explains how type and grade determine the right treatment approach.
- Above the dentate line: Rectum (lined with rectal mucosa—same tissue that lines your intestines)
- Below the dentate line: Anal canal (lined with skin—modified skin, but skin nonetheless)
This seemingly minor distinction creates a massive difference in how hemorrhoids feel and behave.
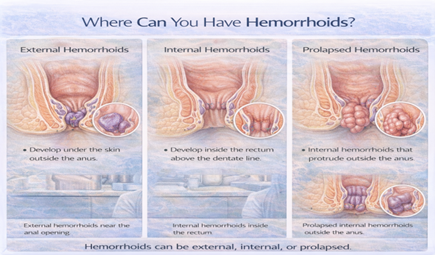
Internal Hemorrhoids: Above the Dentate Line
Location: Inside the rectum, above the dentate line
Tissue type: Covered by rectal mucosa
Critical feature: Rectal mucosa has NO pain receptors (no sensory nerves for pain)
What this means:
- Internal hemorrhoids typically don’t hurt (even when they’re large or bleeding)
- You usually can’t see or feel them (they’re inside the rectum)
- When they bleed, it’s painless bleeding
- When they prolapse (come out), you feel pressure or fullness, but not sharp pain
External Hemorrhoids: Below the Dentate Line
Location: Under the skin around the anus, below the dentate line
Tissue type: Covered by skin (modified anal skin, but with pain receptors)
Critical feature: Skin has abundant pain receptors
What this means:
- External hemorrhoids can be painful (especially if thrombosed—clotted)
- You can see and feel them (visible lumps around the anus)
- They rarely bleed (unless irritated or scratched)
- When they swell or clot, they hurt significantly
The Simple Rule:
- Internal hemorrhoids = Inside the rectum = No pain receptors =
Experiencing symptoms like these? A discreet same-day specialist assessment is available across Dubai.
WhatsApp: +971 55 318 8469 | Phone: +971 55 318 8469
Medcare Discovery Gardens (Dubai)
Bleed but don’t hurt
- External hemorrhoids = Under the skin = Pain receptors present =
Hurt but rarely bleed
Internal Hemorrhoids: Symptoms and What to Expect
How They Present:
1. Painless Bleeding
- Bright red blood on toilet paper, in the bowl, or on the surface of stool
- Happens during or immediately after bowel movements
- Amount varies from streaks to several tablespoons
- No pain associated with the bleeding
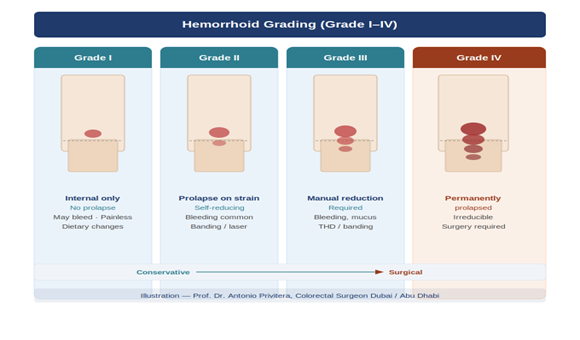
2. Prolapse (Coming Out)
- Depending on grade (I-IV), internal hemorrhoids can prolapse through the anus
- Grade I: Don’t prolapse—stay inside, only symptom is bleeding
- Grade II: Prolapse during straining, go back in automatically
- Grade III: Prolapse during bowel movements, require manual reduction (you push them back in)
- Grade IV: Permanently prolapsed, cannot be pushed back in
3. Mucus Discharge
- Prolapsing internal hemorrhoids can leak mucus
- Causes itching, irritation, dampness
- May lead to minor soiling of underwear
4. Feeling of Incomplete Evacuation
- Large internal hemorrhoids can make you feel like you haven’t fully emptied your bowels
- Sensation of “something still there” after a bowel movement
What You Usually DON’T Feel with Internal Hemorrhoids:
- Sharp pain (unless they become strangulated—blood supply cut off, which is rare)
- Pain during bowel movements (bleeding is painless)
- Constant discomfort (most internal hemorrhoids are symptom-free between bowel movements)
When Internal Hemorrhoids DO Hurt:
There are two scenarios where internal hemorrhoids cause pain:
1. Strangulated Internal Hemorrhoid
- A prolapsed internal hemorrhoid gets trapped outside the anus
- Blood supply is cut off
- Tissue becomes swollen, purple, and painful
- This is uncommon and requires urgent treatment
2. When Internal Hemorrhoids Have External Component (Mixed Hemorrhoids)
- If there’s an external hemorrhoid component, that part can hurt
- See “Mixed Hemorrhoids” section below
External Hemorrhoids: Symptoms and What to Expect
How They Present:
1. Visible/Palpable Lump
- You can see a soft lump or swelling around the anus
- You can feel it when wiping or touching the area
- Usually skin-colored, sometimes slightly blue or purple
2. Discomfort or Pain
- Mild: General discomfort, especially when sitting or during bowel movements
- Moderate: Aching or soreness around the anus
- Severe: If thrombosed (clotted), can be very painful for 48-72 hours
3. Itching or Irritation
- The skin around external hemorrhoids can become irritated
- Moisture or difficulty cleaning the area can worsen itching
4. Skin Tags
- After an external hemorrhoid swells and then resolves, you may be left with a skin tag (excess skin)
- Skin tags themselves are painless but can make cleaning difficult or be cosmetically bothersome
Thrombosed External Hemorrhoid (Special Case):
This is when a blood clot forms inside an external hemorrhoid:
- Sudden onset: Appears over hours, often after straining or heavy lifting
- Severe pain: Throbbing, constant pain (worst in first 48-72 hours)
- Visible lump: Firm, tender, blue or purple lump near anus
- Treatment window: Best treated within 48-72 hours by excising
(removing) the clot under local anesthesia
We covered this in detail in our thrombosed hemorrhoid emergency
What You Usually DON’T Get with External Hemorrhoids:
- Bleeding (unless you scratch or irritate them)
- Prolapse (they’re already outside—they don’t come in and out like internal ones)
- Mucus discharge (that’s an internal hemorrhoid symptom)
Mixed Hemorrhoids: When You Have Both
Many patients—especially those with Grade III or IV disease—have
mixed hemorrhoids: both internal and external components.
How Mixed Hemorrhoids Present:
- Bleeding from the internal component (painless, bright red)
- Pain or discomfort from the external component
- Prolapse of the internal hemorrhoid, with visible external tissue around it
- Combination symptoms: You might bleed painlessly most of the time, but feel pain or pressure when the hemorrhoid prolapsed
Why This Confuses Patients:
A patient comes in and says: “My doctor told me I have internal
hemorrhoids, but I can feel a lump outside—how is that internal?”
Answer: When an internal hemorrhoid prolapses (comes out through the anus), you can see and feel it outside. But it’s still an internal hemorrhoid that has prolapsed—it originated above the dentate line.
The lump you feel outside could be:
1. A prolapsed internal hemorrhoid (soft, reddish, covered with mucosa)
2. An external hemorrhoid (firmer, skin-colored, covered with skin)
3. Both (mixed hemorrhoids—internal hemorrhoid prolapsing with external component around it)
This is why proper examination (anoscopy) is essential—symptoms alone can’t always distinguish between internal, external, and mixed.
Treatment Differences: Why Hemorrhoid Type Matters
The type of hemorrhoid determines which treatments are appropriate:
Treatment for Internal Hemorrhoids:
Grade I-II:
- Conservative treatment (fiber, hydration, bowel habits) Rubber band ligation(office procedure) Sclerotherapy or infrared coagulation
Grade II-III:
- Rubber band ligation (may require multiple sessions)
- Laser hemorrhoidoplasty
- THD (Transanal Hemorrhoidal Dearterialization)
Grade IV:
- Usually requires hemorrhoidectomy (surgical excision)
- THD possible if minimal external component
Key point: Office procedures (banding) and minimally invasive OR procedures (laser, THD) work for internal hemorrhoids. They don’t treat external components.
Treatment for External Hemorrhoids:
Small, Asymptomatic External Hemorrhoids:
- Often need no treatment
- Conservative care (prevent irritation, good hygiene)
Symptomatic External Hemorrhoids or Skin Tags:
- Excision (surgical removal) if bothersome
- Usually done under local anesthesia in office or minor OR procedure
Thrombosed External Hemorrhoid:
- Within 48-72 hours: Excision under local anesthesia provides immediate relief
- After 72 hours: Conservative management (ice, pain relief, sitz baths) as clot is already resolving
Key point: External hemorrhoids and skin tags can’t be treated with banding, laser, or THD—they require excision.
If symptoms persist or are not improving, a specialist assessment in Dubai can help determine the most appropriate treatment.
Treatment for Mixed Hemorrhoids:
When you have both internal and external components:
Option 1: Staged Treatment
- Treat internal component first (banding, laser, or THD)
- Address external component separately if it remains symptomatic
Option 2: Combined Treatment
- Hemorrhoidectomy treats both internal and external components at once
- More invasive, longer recovery, but addresses everything in one procedure
Option 3: Internal Only
- If external component is small and asymptomatic, treat internal only External skin tags can be left alone if not bothersome
How We Diagnose: Examination Is Essential
You cannot reliably distinguish internal from external hemorrhoids based on symptoms alone. Proper diagnosis requires examination:
Visual Inspection:
- Identifies external hemorrhoids, skin tags, fissures Shows prolapsed internal hemorrhoids (if currently prolapsed)
Digital Rectal Exam:
- Feels for masses in the lower rectum
- Assesses sphincter tone
Anoscopy (Most Important for Internal Hemorrhoids):
- A small, lighted scope inserted a few centimeters into the anus
- Directly visualizes internal hemorrhoids
- Determines hemorrhoid grade (I-IV)
- Identifies bleeding source
Without anoscopy, internal hemorrhoids are invisible. You can’t see them with visual inspection alone, and you can’t feel them with digital exam alone (they’re too soft). This is why I insist on anoscopy before recommending treatment—I need to see what we’re dealing with.
Common Misconceptions and Confusions
Misconception #1: “If I can feel a lump, it must be external”
Reality: You might be feeling:
- A prolapsed internal hemorrhoid (Grade II, III, or IV)
- An external hemorrhoid
- Both (mixed hemorrhoids)
Only examination can distinguish.
Misconception #2: “External hemorrhoids always hurt”
Reality: Small external hemorrhoids are often painless. They only
hurt if:
- Thrombosed (clotted)
- Irritated or inflamed
- Large enough to cause pressure
Many external hemorrhoids and skin tags cause no symptoms at all.
Misconception #3: “If it’s bleeding, it can’t be external”
Reality: While internal hemorrhoids are the most common source of bleeding, external hemorrhoids can bleed if:
- Scratched or traumatized
- Thrombosed hemorrhoid ruptures (releases clot and blood)
- Skin is irritated from wiping
However, painless, spontaneous bleeding during bowel movements is almost always from internal hemorrhoids.
Misconception #4: “Internal hemorrhoids can’t be painful”
Reality: Usually true, but exceptions:
- Strangulated internal hemorrhoid (prolapsed with blood supply cut off)
- Mixed hemorrhoids (internal + external, the external part hurts)
- Thrombosed prolapsed internal hemorrhoid
If you have an internal hemorrhoid and it hurts, something unusual is happening—seek evaluation.
Misconception #5: “I can push an external hemorrhoid back in”
Reality: External hemorrhoids are under the skin—they don’t go “back in” because they were never “inside.”
What you CAN push back in is a prolapsed internal hemorrhoid (Grade III). Once you push it in, it stays inside until the next bowel movement. Grade IV prolapsed hemorrhoids cannot be pushed back in at all.
When to Seek Treatment
For Internal Hemorrhoids, Seek Treatment If:
- Bleeding persists for more than 1-2 weeks
- Bleeding is heavy or frequent
- You’re developing anemia (fatigue, weakness, pale skin)
- Prolapse is worsening (Grade III or IV)
- Symptoms interfere with quality of life
- You’re 40+ and have never had colon cancer screening (any rectal bleeding warrants colonoscopy)
For External Hemorrhoids, Seek Treatment If:
- Sudden severe pain (possible thrombosed hemorrhoid—best treated within 48-72 hours)
- Chronic discomfort interfering with sitting, work, or activities
- Skin tags make hygiene difficult or are cosmetically bothersome
- You’re concerned about appearance or diagnosis
For Mixed Hemorrhoids:
Usually need treatment if you have symptoms from either component (bleeding from internal, pain from external, or prolapse).
My Approach: Treating What’s Actually There
In my Dubai practice, I see patients every week who were told they had “hemorrhoids” but weren’t told which type or grade. Sometimes they received treatment that didn’t match their anatomy—like banding for primarily external hemorrhoids (which doesn’t work), or being told they need surgery when banding would have sufficed.
Here’s how I approach it:
Step 1: Proper Examination
- Visual inspection (external)
- Digital rectal exam
- Anoscopy (internal)
Step 2: Clear Diagnosis
- “You have Grade II internal hemorrhoids—that’s why you’re bleeding.”
- “You have a thrombosed external hemorrhoid—that’s why it hurts.”
- “You have mixed hemorrhoids: Grade III internal with external component.”
Step 3: Match Treatment to Anatomy
- Internal only → Banding, laser, or THD depending on grade
- External only → Excision if symptomatic
- Mixed → Discuss options (staged treatment vs hemorrhoidectomy)
The key is accuracy. I don’t guess based on symptoms—I examine, diagnose, and then recommend treatment that matches what I actually see.
This article is written and reviewed by Prof. Dr Antonio Privitera, consultant colorectal surgeon with fellowship training at Mayo Clinic (USA) and the Royal College of Surgeons (UK), specializing in hemorrhoid diagnosis and minimally invasive treatment.
Frequently Asked Questions
1. Can internal hemorrhoids become external hemorrhoids?
No. They’re two different anatomical entities based on where they originate relative to the dentate line. However:
Internal hemorrhoids can prolapse (come outside the anus) Chronic prolapse can lead to external skin tags forming around the internal hemorrhoid So you can end up with mixed hemorrhoids, but the internal one
didn’t “turn into” an external one
2. Which type is more serious?
Neither is inherently “more serious.” Both can cause significant symptoms:
Internal hemorrhoids can bleed heavily, prolapse, interfere with life
External hemorrhoids can thrombose and cause severe pain
Mixed hemorrhoids combine both problems
What matters is grade (for internal) and symptoms (for external).
3. Can I have internal hemorrhoids without external ones?
Yes, very common. Many people have only internal hemorrhoids.
4. Can I have external hemorrhoids without internal ones?
Yes, though less common. Some people have only external hemorrhoids or skin tags.
5. Do internal and external hemorrhoids require different diets?
No. Both types benefit from the same preventive measures:
High-fiber diet (25-35g daily)
Adequate hydration (2.5-3 liters daily in Dubai)
Avoiding straining
Regular bowel habits
6. Are external hemorrhoids caused by sitting on cold surfaces?
No. This is a myth. External hemorrhoids are caused by the same factors as internal ones: increased pressure on anal veins from straining, constipation, prolonged sitting, pregnancy, etc. Cold surfaces don’t cause hemorrhoids.
7. If I have a skin tag, does that mean I have external hemorrhoids?
hemorrhoid or thrombosed hemorrhoid that resolved. The skin tag itself is just excess skin—it’s not an active hemorrhoid. However, if it’s bothersome, it can be removed.
8. Can external hemorrhoids be treated with rubber band ligation?
No. Banding only works for internal hemorrhoids (above the dentate line where there are no pain receptors). If you tried to band an external hemorrhoid, it would be excruciatingly painful because the external skin has pain receptors.
9. Why did my doctor say I have internal hemorrhoids when I can feel a lump outside?
The lump you feel is likely a prolapsed internal hemorrhoid—it originated inside (above the dentate line) but has prolapsed through the anus. It’s still classified as an internal hemorrhoid (Grade III or IV depending on whether you can push it back in).
10. I have both internal and external hemorrhoids. Which should be
treated first?
Depends on which is causing more symptoms:
If bleeding from internal hemorrhoids is the main problem → Treat internal first
If pain from external hemorrhoid is the main problem → Treat external first
If both are significantly symptomatic → Consider hemorrhoidectomy (treats both at once)
Your surgeon should discuss the options with you.
The Bottom Line
Understanding the difference between internal and external hemorrhoids helps you:
- Understand your symptoms (bleeding = usually internal; pain = usually external)
- Know what to expect (internal hemorrhoids usually don’t hurt; external ones rarely bleed)
- Choose appropriate treatment (banding for internal, excision for external)
- Have realistic expectations (treating internal hemorrhoids won’t address external skin tags)
But the most important takeaway: You can’t diagnose hemorrhoid type or grade based on symptoms alone. Proper examination (especially anoscopy) is essential for accurate diagnosis and appropriate treatment.
References and Medical Sources
This article is based on anatomical and clinical principles:
1. American Society of Colon and Rectal Surgeons Guidelines – Classification and management of hemorrhoids by type. Davis BR, Lee-Kong SA, Migaly J, Feingold DL, Steele SR. The American Society of Colon and Rectal Surgeons Clinical Practice Guidelines for the Management of Hemorrhoids. Dis Colon Rectum. 2018;61(3):284-292. PubMed
2. Hemorrhoid Anatomy and Classification – Anatomical basis for internal vs external distinction. Lohsiriwat V. Hemorrhoids: from basic pathophysiology to clinical management. World J Gastroenterol. 2012;18(17):2009-2017. PubMed
3. Treatment Approaches Based on Hemorrhoid Type – Evidence-based treatment selection. Garg P, Singh P. Adequate dietary fiber supplement and TONE can help avoid surgery in most patients with advanced hemorrhoids. Minerva Gastroenterol Dietol. 2017;63(2):92-96. PubMed
Medical Review: This content was written and reviewed by Professor training at the Mayo Clinic and Royal College of Surgeons (UK), and European Board Certification in Colorectal Surgery.
Get Proper Diagnosis: Internal, External, or Mixed?
Examination with anoscopy determines hemorrhoid type and grade—then we can recommend the right treatment.
📱 WhatsApp: +971 55 318 8469
📞 Phone: +971 55 318 8469
🌐 Book Online:
Dubai Locations:
- Medcare Medical Centre, Discovery Gardens
- Medcare Women and Children Hospital
- Medcare Royal Specialty Hospital
- Clemenceau Medical Centre
- Aster Hospital, Qusais
Proper examination means proper treatment—matched to your anatomy, not guesswork.
Professor Dr. Antonio Privitera
Fellowship Training: Mayo Clinic | Royal College of Surgeons (UK)
European Board Certified in Colorectal Surgery
About the Author
